

The influence of gut-decontamination prophylactic antibiotics on acute graft-versus-host disease and survival following allogeneic hematopoietic stem cell transplantation
- PMID: 28197380
- PMCID: PMC5283637
- DOI: 10.1080/2162402X.2016.1258506
The influence of gut-decontamination prophylactic antibiotics on acute graft-versus-host disease and survival following allogeneic hematopoietic stem cell transplantation
Abstract
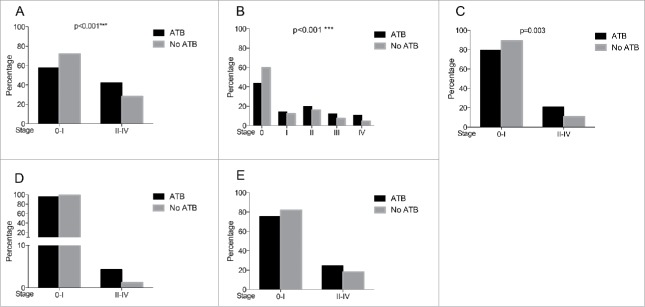
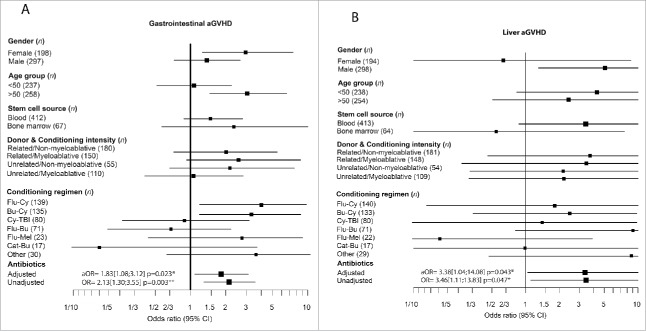
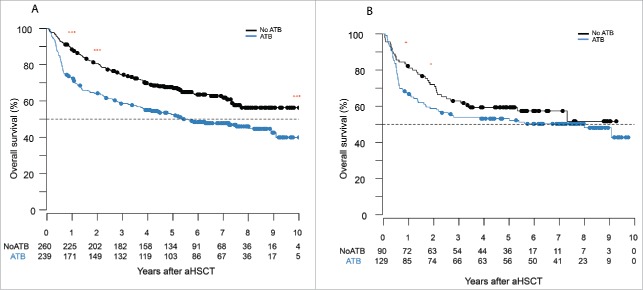
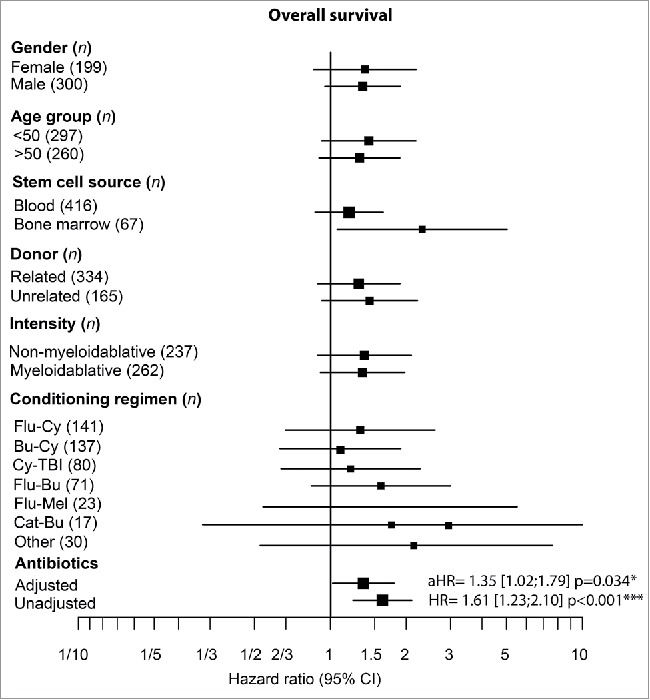
The intestinal microbiota plays a key role in the pathogenesis of acute graft-versus-host disease (aGVHD). High-dose conditioning regimens given prior to allogeneic hematopoietic stem cell transplantation (aHSCT) modulate the composition of gut microbiota and damage the gut epithelial barrier, resulting in increased systemic inflammation. We assessed whether gut decontamination with antibiotics (ATB) prior to aHSCT influenced the frequency of aGVHD and mortality in 500 patients from two Canadian centers between 2005 and 2012. The rate of grade II-IV aGVHD was higher in the ATB arm compared with the arm without ATB (42% vs 28%; p < 0.001). This difference was mainly driven by a 2-fold higher rate of grade II-IV gastrointestinal aGVHD (GI-GVHD) in the ATB arm compared with the arm without ATB (20.7% vs 10.8%; p = 0.003). Multivariate analyses adjusted for known aGVHD risk factors revealed that more patients in the ATB group developed clinically significant GI-GVHD and liver aGVHD; adjusted odds ratio (aOR) = 1.83; p = 0.023 and aOR = 3.56; p = 0.047, respectively. Importantly, median overall survival (OS) was significantly lower in the group receiving ATB and the OS at 10 y remained decreased in the ATB group; adjusted hazard ratio (aHR) = 1.61 (p < 0.001). Without undermining the role of ATB prophylaxis to prevent infection in aHSCT, we have shown that the use of ATB that targets intestinal bacteria is associated with a more severe aGVHD that involves the GI organs and impacts OS. Prospective studies that evaluate the contribution of bacterial decontamination to aGVHD are warranted.
Keywords: Acute graft-versus-host disease; allogeneic hematopoietic stem cell transplantation; antibiotics; gut decontamination; microbiota.
Figures
Similar articles
-
Intestinal Microbiota Can Predict Acute Graft-versus-Host Disease Following Allogeneic Hematopoietic Stem Cell Transplantation.Biol Blood Marrow Transplant. 2019 Oct;25(10):1944-1955. doi: 10.1016/j.bbmt.2019.07.006. Epub 2019 Jul 9. Biol Blood Marrow Transplant. 2019. PMID: 31299215
-
Associations of the gut microbiome and clinical factors with acute GVHD in allogeneic HSCT recipients.Blood Adv. 2020 Nov 24;4(22):5797-5809. doi: 10.1182/bloodadvances.2020002677. Blood Adv. 2020. PMID: 33232475 Free PMC article.
-
Impact of the Use and Type of Antibiotics on Acute Graft-versus-Host Disease.Biol Blood Marrow Transplant. 2018 Nov;24(11):2178-2183. doi: 10.1016/j.bbmt.2018.06.031. Epub 2018 Jul 3. Biol Blood Marrow Transplant. 2018. PMID: 30417828
-
Microbiome: An Emerging New Frontier in Graft-Versus-Host Disease.Dig Dis Sci. 2019 Mar;64(3):669-677. doi: 10.1007/s10620-018-5369-9. Epub 2018 Dec 7. Dig Dis Sci. 2019. PMID: 30523482 Review.
-
The Promise of Precision Nutrition for Modulation of the Gut Microbiota as a Novel Therapeutic Approach to Acute Graft-versus-host Disease.Transplantation. 2023 Dec 1;107(12):2497-2509. doi: 10.1097/TP.0000000000004629. Epub 2023 May 16. Transplantation. 2023. PMID: 37189240 Free PMC article. Review.
Cited by
-
Gut microbiota injury in allogeneic haematopoietic stem cell transplantation.Nat Rev Cancer. 2018 May;18(5):283-295. doi: 10.1038/nrc.2018.10. Epub 2018 Feb 16. Nat Rev Cancer. 2018. PMID: 29449660 Free PMC article. Review.
-
Stool Microbiota at Neutrophil Recovery Is Predictive for Severe Acute Graft vs Host Disease After Hematopoietic Cell Transplantation.Clin Infect Dis. 2017 Nov 29;65(12):1984-1991. doi: 10.1093/cid/cix699. Clin Infect Dis. 2017. PMID: 29020185 Free PMC article.
-
Roles of the intestinal microbiota and microbial metabolites in acute GVHD.Exp Hematol Oncol. 2021 Oct 27;10(1):49. doi: 10.1186/s40164-021-00240-3. Exp Hematol Oncol. 2021. PMID: 34706782 Free PMC article. Review.
-
GPR Expression in Intestinal Biopsies From SCT Patients Is Upregulated in GvHD and Is Suppressed by Broad-Spectrum Antibiotics.Front Immunol. 2021 Oct 28;12:753287. doi: 10.3389/fimmu.2021.753287. eCollection 2021. Front Immunol. 2021. PMID: 34777363 Free PMC article.
-
Microbiota in cancer development and treatment.J Cancer Res Clin Oncol. 2019 Jan;145(1):49-63. doi: 10.1007/s00432-018-2816-0. Epub 2018 Dec 12. J Cancer Res Clin Oncol. 2019. PMID: 30542789 Free PMC article. Review.
References
-
- Sender R, Fuchs S, Milo R. Are we really vastly outnumbered? Revisiting the ratio of bacterial to host cells in humans. Cell 2016; 164:337-40; PMID:26824647; http://dx.doi.org/ 10.1016/j.cell.2016.01.013 - DOI - PubMed
-
- Garrett WS. Cancer and the microbiota. Science 2015; 348:80-6; PMID:25838377; http://dx.doi.org/ 10.1126/science.aaa4972 - DOI - PMC - PubMed
-
- Zitvogel L, Ayyoub M, Routy B, Kroemer G. Microbiome and anticancer immunosurveillance. Cell 2016; 165:276-87; PMID:27058662; http://dx.doi.org/11413166 10.1016/j.cell.2016.03.001 - DOI - PubMed
-
- Cooke KR, Gerbitz A, Crawford JM, Teshima T, Hill GR, Tesolin A, Rossignol DP, Ferrara JL. LPS antagonism reduces graft-versus-host disease and preserves graft-versus-leukemia activity after experimental bone marrow transplantation. J Clin Invest 2001; 107:1581-9 PMID:11413166; http://dx.doi.org/ 10.1172/JCI12156 - DOI - PMC - PubMed
-
- Zeiser R, Socie G, Blazar BR. Pathogenesis of acute graft-versus-host disease: from intestinal microbiota alterations to donor T cell activation. Br J Haematol 2016; 175:191-207; PMID:27619472; http://dx.doi.org/ 10.1111/bjh.14295 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources