

Radiological findings of unilateral tuberculous lung destruction
- PMID: 28197882
- PMCID: PMC5359149
- DOI: 10.1007/s13244-017-0547-4
Radiological findings of unilateral tuberculous lung destruction
Abstract
Objectives: The aim of this report is to identify the radiological findings of unilateral tuberculous lung destruction (UTLD).
Materials and methods: Thirteen patients with (UTLD) were reviewed from 1999 to 2014. Only patients with radiological evidence of absence of pulmonary parenchyma preserved were included. Clinical and demographic data were obtained and radiological studies (chest radiograph and CT) were retrospectively reviewed.
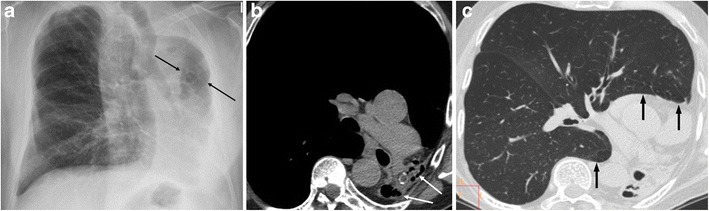
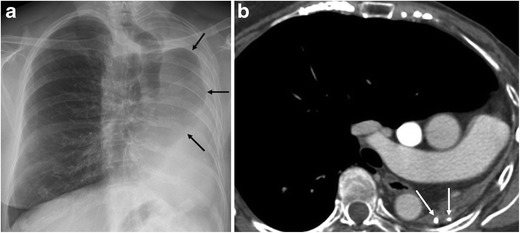
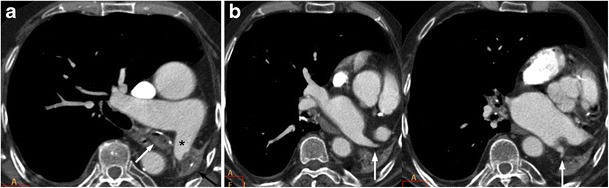
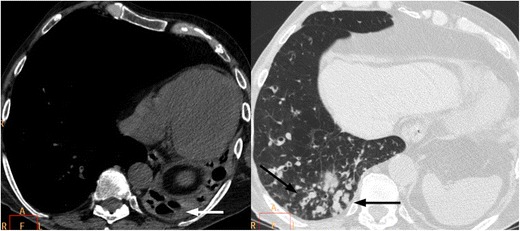
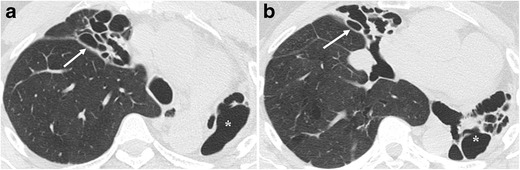
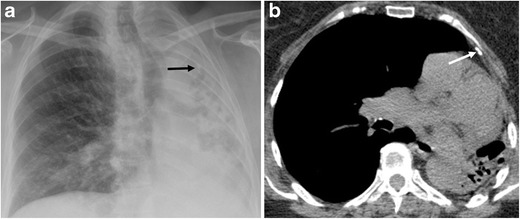
Results: The left lung was more commonly involved (85%). The following radiological findings were found in all cases: a decrease in the diameter of the pulmonary vessels of the affected lung, herniation of the contralateral lung and hypertrophy of the ribs and/or thickening of extrapleural fat. Two radiological patterns were identified: UTLD with cystic bronchiectasis (85%) and UTLD without residual cystic bronchiectasis (15%). Forty-six per cent of cases had respiratory infection symptoms with presence of air-fluid levels in the affected lung as the most common finding in these patients.
Conclusions: Total unilateral post-tuberculous lung destruction is an irreversible complication with the following main radiological features: predominantly left-sided location, decreases in the diameter of the ipsilateral pulmonary vessels, herniation of the contralateral lung and hypertrophy of the ribs and/or thickening of extrapleural fat.
Teaching points: • Unilateral tuberculous lung destruction is an irreversible complication of tuberculosis. • Left-side predominance and herniation of the contralateral lung are characteristic. • Decreased diameter of the ipsilateral pulmonary vessels occurred in all patients. • The pattern with residual cystic bronchiectasis is the most frequent. • Superimposed non-tuberculous infections may affect the destroyed lung.
Keywords: CT scanner, X-ray; Infections, respiratory; Radiography; Thoracic; Tuberculosis, pulmonary.
Figures

References
-
- World Health Organization (2016) Global tuberculosis report 2015. World Health Organization, Geneva. Available via http://www.who.int/tb/publications/global_report/gtbr15_main_text.pdf?ua=1. Accessed 5 Aug 2016
-
- Fawibe AE, et al. Profile and outcome of unilateral tuberculous lung destruction in Ilorin, Nigeria. West Afr J Med. 2011;30(2):130–135. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
