

Child Growth According to Maternal and Child HIV Status in Zimbabwe
- PMID: 28198792
- PMCID: PMC5571879
- DOI: 10.1097/INF.0000000000001574
Child Growth According to Maternal and Child HIV Status in Zimbabwe
Abstract
Background: Growth failure is common among HIV-infected infants, but there are limited data on the effects of HIV exposure or timing of HIV acquisition on growth.
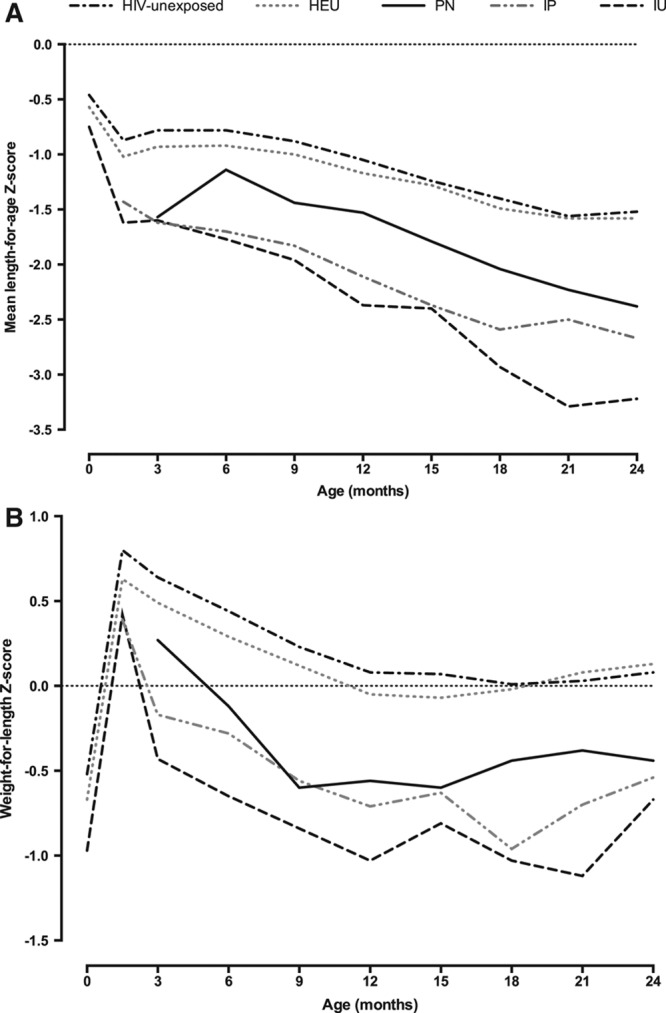
Methods: Fourteen thousand one hundred ten infants were enrolled in the Zimbabwe Vitamin A for Mothers and Babies trial in Zimbabwe before the availability of antiretroviral therapy or co-trimoxazole. Anthropometric measurements were taken from birth through 12-24 months of age. Growth outcomes were compared between 5 groups of children: HIV-infected in utero (IU), intrapartum (IP) or postnatally (PN); HIV-exposed uninfected (HEU); and HIV unexposed.
Results: Growth failure was common across all groups of children. Compared with HIV-unexposed children, IU-, IP- and PN-infected children had significantly lower length-for-age and weight-for-length Z scores throughout the first 2 years of life. At 12 months, odds ratios for stunting were higher in IU [6.25, 95% confidence interval (CI): 4.20-9.31] and IP infants (4.76, 95% CI: 3.58-6.33) than in PN infants (1.70, 95% CI: 1.16-2.47). Compared with HIV-unexposed infants, HEU infants at 12 months had odds ratios for stunting of 1.23 (95% CI: 1.08-1.39) and wasting of 1.56 (95% CI: 1.22-2.00).
Conclusions: HIV-infected infants had very high rates of growth failure during the first 2 years of life, particularly if IU or IP infected, highlighting the importance of early infant diagnosis and antiretroviral therapy. HEU infants had poorer growth than HIV-unexposed infants in the first 12 months of life.
Figures
References
-
- World Health Organization. Global Update on the Health Sector Response to HIV, 2014. 2014Geneva: World Health Organization.
-
- Datta P, Embree JE, Kreiss JK, et al. Mother-to-child transmission of human immunodeficiency virus type 1: report from the Nairobi Study. J Infect Dis. 1994;170:1134–1140.. - PubMed
-
- O’Brien DP, Sauvageot D, Zachariah R, et al. ; Medecins Sans Frontieres. In resource-limited settings good early outcomes can be achieved in children using adult fixed-dose combination antiretroviral therapy. AIDS. 2006;20:1955–1960.. - PubMed
-
- Marinda E, Humphrey JH, Iliff PJ, et al. ; ZVITAMBO Study Group. Child mortality according to maternal and infant HIV status in Zimbabwe. Pediatr Infect Dis J. 2007;26:519–526.. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
