

Comparison of the population excess fraction of Chlamydia trachomatis infection on pelvic inflammatory disease at 12-months in the presence and absence of chlamydia testing and treatment: Systematic review and retrospective cohort analysis
- PMID: 28199392
- PMCID: PMC5310913
- DOI: 10.1371/journal.pone.0171551
Comparison of the population excess fraction of Chlamydia trachomatis infection on pelvic inflammatory disease at 12-months in the presence and absence of chlamydia testing and treatment: Systematic review and retrospective cohort analysis
Abstract
Background: The impact of Chlamydia trachomatis (chlamydia) control on the incidence of pelvic inflammatory disease (PID) is theoretically limited by the proportion of PID caused by chlamydia. We estimate the population excess fraction (PEF) of treated chlamydia infection on PID at 12-months in settings with widespread chlamydia control (testing and treatment) and compare this to the estimated PEF of untreated chlamydia.
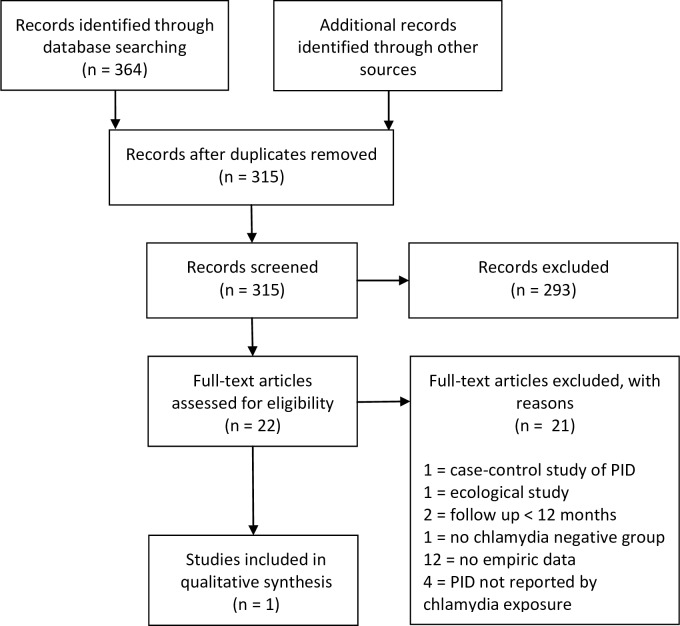
Methods: We used two large retrospective population-based cohorts of women of reproductive age from settings with widespread chlamydia control to calculate the PEF of treated chlamydia on PID at 12-months. We undertook a systematic review to identify further studies that reported the risk of PID in women who were tested for chlamydia (infected and uninfected). We used the same method to calculate the PEF in eligible studies then compared all estimates of PEF.
Results: The systematic review identified a single study, a randomised controlled trial of chlamydia screening (POPI-RCT). In the presence of testing and treatment <10% of PID at 12-months was attributable to treated (baseline) chlamydia infections (Manitoba: 8.86%(95%CI 7.15-10.75); Denmark: 3.84%(3.26-4.45); screened-arm POPI-RCT: 0.99%(0.00-29.06)). In the absence of active chlamydia treatment 26.44%(11.57-46.32) of PID at 12-months was attributable to untreated (baseline) chlamydia infections (deferred-arm POPI-RCT). The PEFs suggest that eradicating baseline chlamydia infections could prevent 484 cases of PID at 12-months per 100,000 women in the untreated setting and 13-184 cases of PID per 100,000 tested women in the presence of testing and treatment.
Conclusion: Testing and treating chlamydia reduced the PEF of chlamydia on PID by 65% compared to the untreated setting. But in the presence of testing and treatment over 90% of PID could not be attributed to a baseline chlamydia infection. More information is needed about the aetiology of PID to develop effective strategies for improving the reproductive health of women.
Conflict of interest statement
Figures
References
-
- European Centre for Disease Control and Prevention. Chlamydia control in Europe: literature review. Stockholm ECDC, 2014 February 2014. Report No.
-
- European Centre for Disease Control and Prevention. Chlamydia control in Europe: a survey of Member States 2012. Stockholm ECDC, 2014 February 2014. Report No.
-
- Price MJ, Ades AE, Soldan K, Welton NJ, Macleod J, Simms I, et al. The natural history of Chlamydia trachomatis infection in women: a multi-parameter evidence synthesis. Health technology assessment (Winchester, England). 2016;20(22):1–250. Epub 2016/03/24. PubMed Central PMCID: PMCPmc4819202. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
