

Cortical porosity not superior to conventional densitometry in identifying hemodialysis patients with fragility fracture
- PMID: 28199411
- PMCID: PMC5310770
- DOI: 10.1371/journal.pone.0171873
Cortical porosity not superior to conventional densitometry in identifying hemodialysis patients with fragility fracture
Abstract
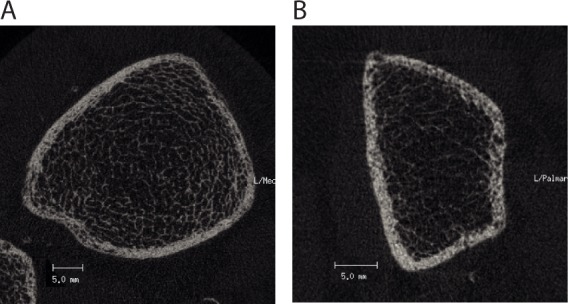
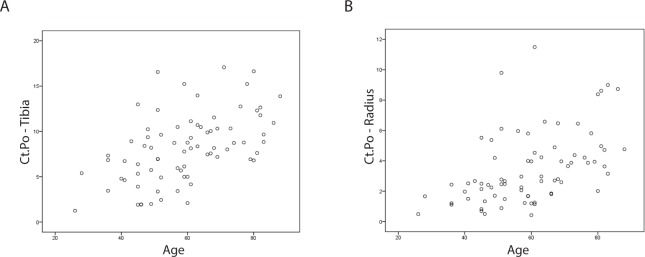
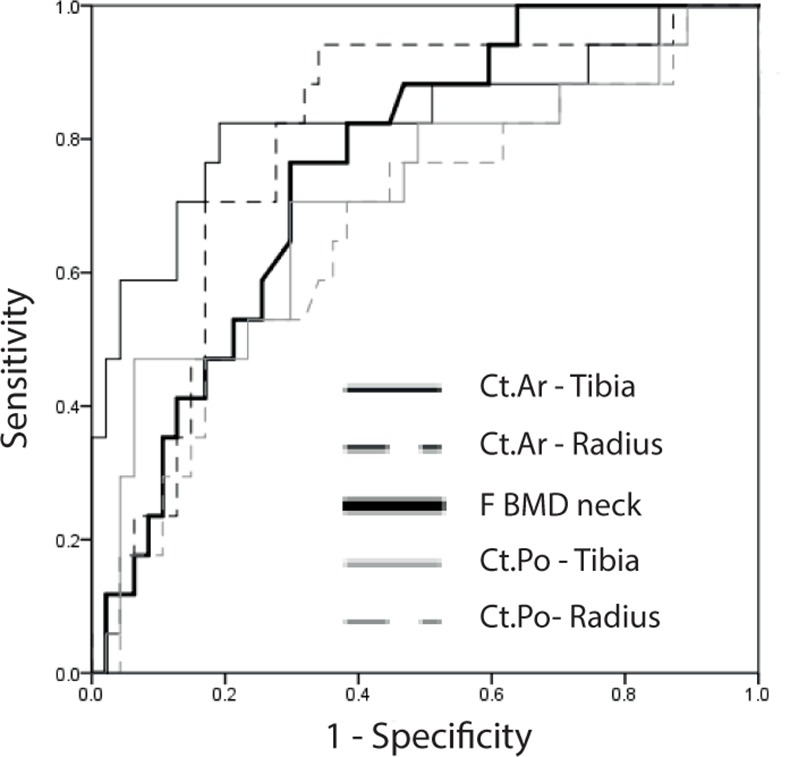
Hemodialysis (HD) patients face increased fracture risk, which is further associated with elevated risk of hospitalization and mortality. High-resolution peripheral computed tomography (HR-pQCT) has advanced our understanding of bone disease in chronic kidney disease by characterizing distinct changes in both the cortical and trabecular compartments. Increased cortical porosity (Ct.Po) has been shown to be associated with fracture in patients with osteopenia or in postmenopausal diabetic women. We tested whether the degree of Ct.Po identifies hemodialysis patients with prevalent fragility fractures in comparison to bone mineral density (BMD) assessed by dual X-ray absorptiometry (DXA). We performed a post-hoc analysis of a cross-sectional study in 76 prevalent hemodialysis patients. Markers of mineral metabolism, coronary calcification score, DXA-, and HR-pQCT-data were analyzed, and Ct.Po determined at radius and tibia. Ct.Po was significantly higher in patients with fracture but association was lost after adjusting for age and gender (tibia p = 0.228, radius p = 0.5). Instead, femoral (F) BMD neck area (p = 0.03), F T-score neck area (p = 0.03), radius (R) BMD (p = 0.03), R T-score (p = 0.03), and cortical HR-pQCT indices such as cortical area (Ct.Ar) (tibia: p = 0.01; radius: p = 0.02) and cortical thickness (Ct.Th) (tibia: p = 0.03; radius: p = 0.02) correctly classified patients with fragility fractures. Area under receiver operating characteristic curves (AUC) for Ct.Po (tibia AUC: 0.711; p = 0.01; radius AUC: 0.666; p = 0.04), Ct.Ar (tibia AUC: 0.832; p<0.001; radius AUC: 0.796; p<0.001), and F neck BMD (AUC: 0.758; p = 0.002) did not differ significantly among each other. In conclusion, measuring Ct.Po is not superior to BMD determined by DXA for identification of HD patients with fragility fracture.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
