

The Hotel Study-Clinical and Health Service Effectiveness in a Cohort of Homeless or Marginally Housed Persons
- PMID: 28199798
- PMCID: PMC5528984
- DOI: 10.1177/0706743717693781
The Hotel Study-Clinical and Health Service Effectiveness in a Cohort of Homeless or Marginally Housed Persons
Abstract
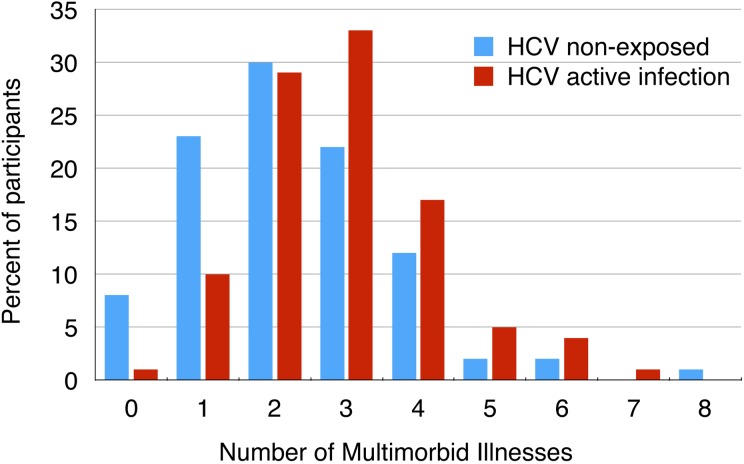
Objective: The Hotel Study was initiated in Vancouver's Downtown East Side (DTES) neighborhood to investigate multimorbidity in homeless or marginally housed people. We evaluated the clinical effectiveness of existing, illness-specific treatment strategies and assessed the effectiveness of health care delivery for multimorbid illnesses.
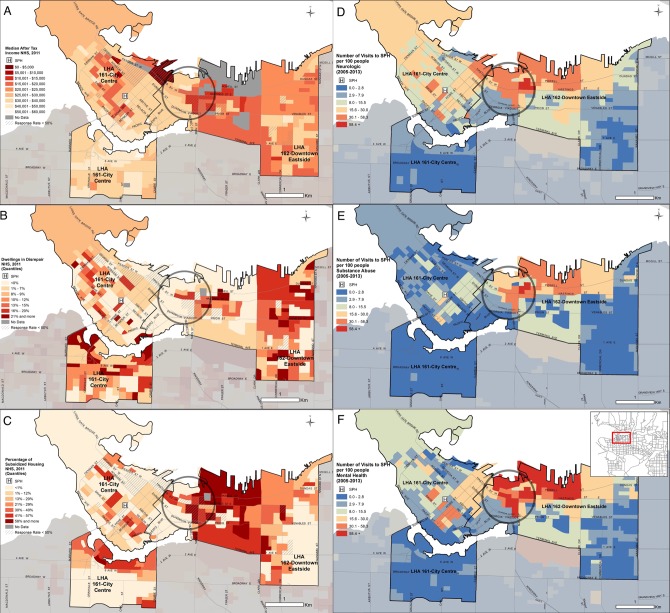
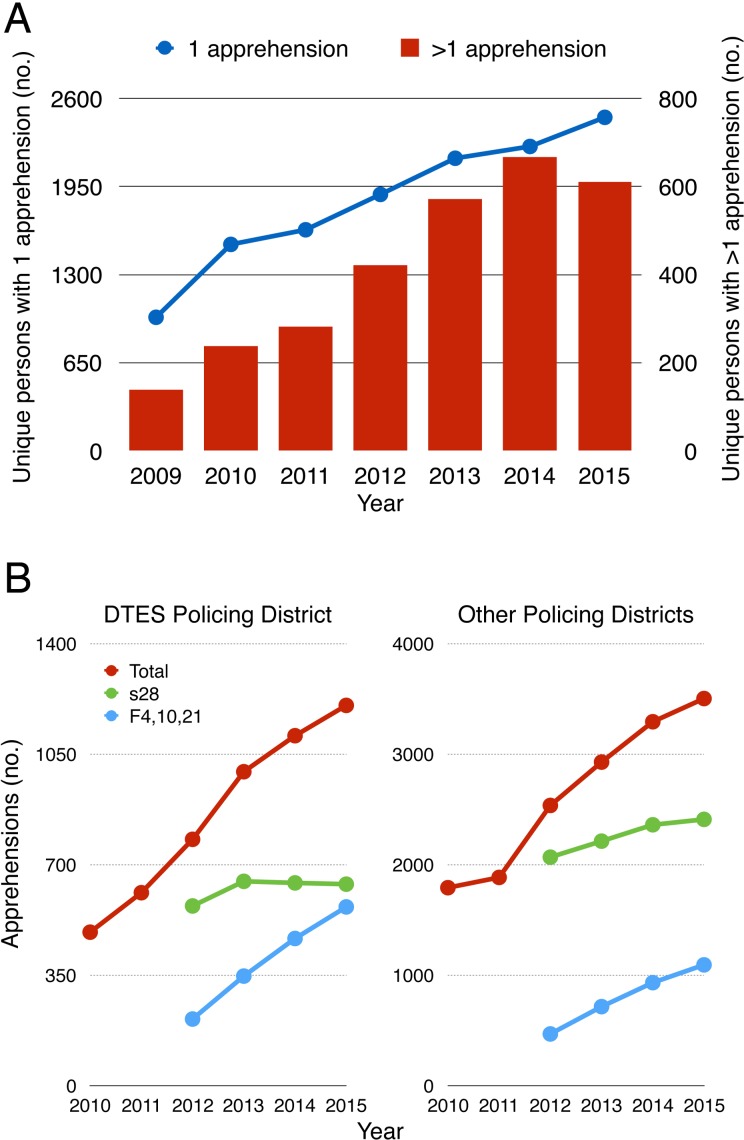
Method: For context, we mapped the housing locations of patients presenting for 552,062 visits to the catchment hospital emergency department (2005-2013). Aggregate data on 22,519 apprehensions of mentally ill people were provided by the Vancouver Police Department (2009-2015). The primary strategy was a longitudinal cohort study of 375 people living in the DTES (2008-2015). We analysed mortality and evaluated the clinical and health service delivery effectiveness for infection with human immunodeficiency virus or hepatitis C virus, opioid dependence, and psychosis.
Results: Mapping confirmed the association between poverty and greater number of emergency visits related to substance use and mental illness. The annual change in police apprehensions did not differ between the DTES and other policing districts. During 1581 person-years of cohort observation, the standardized mortality ratio was 8.43 (95% confidence interval, 6.19 to 11.50). Physician visits were common (84.3% of participants over 6 months). Clinical treatment effectiveness was highest for HIV/AIDS, intermediate for opioid dependence, and lowest for psychosis. Health service delivery mechanisms provided examples of poor access, poor treatment adherence, and little effect on multimorbid illnesses.
Conclusions: Clinical effectiveness was variable, and illness-specific service delivery appeared to have little effect on multimorbidity. New models of care may need to be implemented.
Objectif:: L’étude Hotel a débuté dans le quartier Downtown East Side (DTES) de Vancouver pour mener une recherche sur la multi-morbidité chez les personnes sans abri ou ayant un logement précaire. Nous avons évalué l’efficacité clinique des stratégies existantes de traitement de maladies spécifiques et évalué l’efficacité de la prestation des soins de santé pour les maladies multi-morbides.
Méthode:: Pour le contexte, nous avons configuré les lieux où logent des patients qui se sont présentés 552 062 fois au service d’urgence de l’hôpital de la zone couverte (2005-2013). Les données agrégées de 22 519 arrestations de personnes souffrant de maladie mentale ont été fournies par le service de police de Vancouver (2009-2015). La stratégie principale était une étude de cohorte longitudinale de 375 personnes vivant dans le DTES (2008-2015). Nous avons analysé la mortalité, et évalué l’efficacité de la prestation des services de santé et cliniques pour : l’infection à virus de l’immunodéficience humaine ou à virus de l’hépatite C, la dépendance aux opioïdes, et la psychose.
Résultats:: La configuration a confirmé l’association entre la pauvreté et le plus grand nombre de visites à l’urgence liées à l’utilisation de substances et à la maladie mentale. Le changement annuel des arrestations de la police ne différait pas entre le DTES et d’autres districts de police. Durant 1581 années-personnes d’observation de cohorte, le taux de mortalité normalisé était de 8,43 (intervalle de confiance à 95 % 6,19 à 11,50). Les visites à un médecin étaient fréquentes (84,3 % des participants sur 6 mois). L’efficacité du traitement clinique était la plus élevée pour le VIH/sida, intermédiaire pour la dépendance aux opioïdes, et faible pour la psychose. Les mécanismes de la prestation de services ont présenté des exemples de mauvais accès, de médiocre observance du traitement, et de peu d’effet sur les maladies multi-morbides.
Conclusions:: L’efficacité clinique était variable, et la prestation de services pour les maladies spécifiques semblait avoir peu d’effet sur la multi-morbidité. Il faut peut-être mettre en œuvre de nouveaux modèles de soins.
Keywords: HCV; HIV; heroin; mortality; multimorbidity; police; psychosis.
Conflict of interest statement
Figures
References
-
- Economist Data Team. The world’s most “liveable” cities. Economist. 2015;1–3. Available from: http://www.economist.com/blogs/graphicdetail/2015/08/daily-chart-5
-
- Hwang SW, Aubry T, Palepu A, et al. The health and housing in transition study: a longitudinal study of the health of homeless and vulnerably housed adults in three Canadian cities. Int J Public Health. 2011;56(6):609–623. - PubMed
-
- Ganesh A, Campbell DJT, Hurley J, et al. High positive psychiatric screening rates in an urban homeless population. Can J Psychiatry. 2013;58(6):353–360. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
