

Opioid-Prescribing Patterns of Emergency Physicians and Risk of Long-Term Use
- PMID: 28199807
- PMCID: PMC5428548
- DOI: 10.1056/NEJMsa1610524
Opioid-Prescribing Patterns of Emergency Physicians and Risk of Long-Term Use
Abstract
Background: Increasing overuse of opioids in the United States may be driven in part by physician prescribing. However, the extent to which individual physicians vary in opioid prescribing and the implications of that variation for long-term opioid use and adverse outcomes in patients are unknown.
Methods: We performed a retrospective analysis involving Medicare beneficiaries who had an index emergency department visit in the period from 2008 through 2011 and had not received prescriptions for opioids within 6 months before that visit. After identifying the emergency physicians within a hospital who cared for the patients, we categorized the physicians as being high-intensity or low-intensity opioid prescribers according to relative quartiles of prescribing rates within the same hospital. We compared rates of long-term opioid use, defined as 6 months of days supplied, in the 12 months after a visit to the emergency department among patients treated by high-intensity or low-intensity prescribers, with adjustment for patient characteristics.
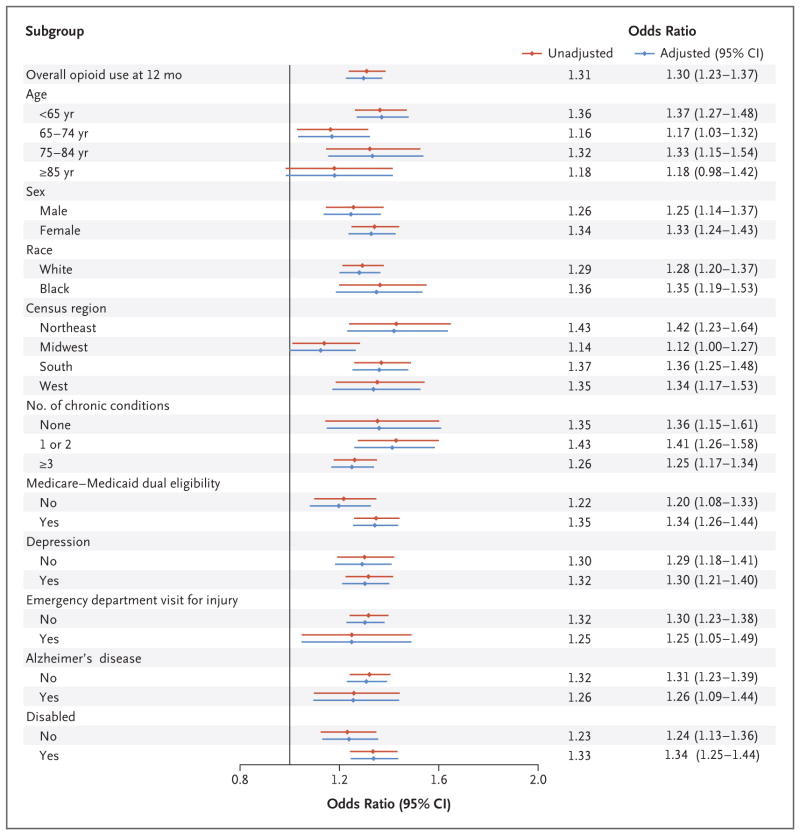
Results: Our sample consisted of 215,678 patients who received treatment from low-intensity prescribers and 161,951 patients who received treatment from high-intensity prescribers. Patient characteristics, including diagnoses in the emergency department, were similar in the two treatment groups. Within individual hospitals, rates of opioid prescribing varied widely between low-intensity and high-intensity prescribers (7.3% vs. 24.1%). Long-term opioid use was significantly higher among patients treated by high-intensity prescribers than among patients treated by low-intensity prescribers (adjusted odds ratio, 1.30; 95% confidence interval, 1.23 to 1.37; P<0.001); these findings were consistent across multiple sensitivity analyses.
Conclusions: Wide variation in rates of opioid prescribing existed among physicians practicing within the same emergency department, and rates of long-term opioid use were increased among patients who had not previously received opioids and received treatment from high-intensity opioid prescribers. (Funded by the National Institutes of Health.).
Figures

Comment in
-
Opioid Prescribing by Emergency Physicians and Risk of Long-Term Use.N Engl J Med. 2017 May 11;376(19):1895. doi: 10.1056/NEJMc1703338. N Engl J Med. 2017. PMID: 28489998 Free PMC article. No abstract available.
-
Opioid Prescribing by Emergency Physicians and Risk of Long-Term Use.N Engl J Med. 2017 May 11;376(19):1895-6. doi: 10.1056/NEJMc1703338. N Engl J Med. 2017. PMID: 28492072 No abstract available.
-
Creating opioid dependence in the emergency department.CJEM. 2018 Jan;20(1):100-103. doi: 10.1017/cem.2017.370. Epub 2017 Sep 29. CJEM. 2018. PMID: 28958216
References
-
- Vital signs: overdoses of prescription opioid pain relievers — United States, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60:1487–2. - PubMed
-
- Prescription opioid overdose data. Atlanta: Centers for Disease Control and Prevention; 2016. ( http://www.cdc.gov/drugoverdose/data/overdose.html)
-
- National Institute on Drug Abuse. America’s addiction to opioids: heroin and prescription drug abuse. 2014 May 14; ( https://www.drugabuse.gov/about-nida/legislative-activities/testimony-to...)
-
- Healthcare Cost and Utilization Project. Hospital inpatient utilization related to opioid overuse among adults, 1993–2012. 2014 Aug; ( https://www.hcup-us.ahrq.gov/reports/statbriefs/sb177-Hospitalizations-f...) - PubMed
-
- Vestal C. Older addicts squeezed by opioid epidemic. Stateline. 2016 Jul 26; ( http://pew.org/2asv3TO)
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources