

Preclinical Efficacy Failure of Human CNS-Derived Stem Cells for Use in the Pathway Study of Cervical Spinal Cord Injury
- PMID: 28199829
- PMCID: PMC5312249
- DOI: 10.1016/j.stemcr.2016.12.018
Preclinical Efficacy Failure of Human CNS-Derived Stem Cells for Use in the Pathway Study of Cervical Spinal Cord Injury
Abstract
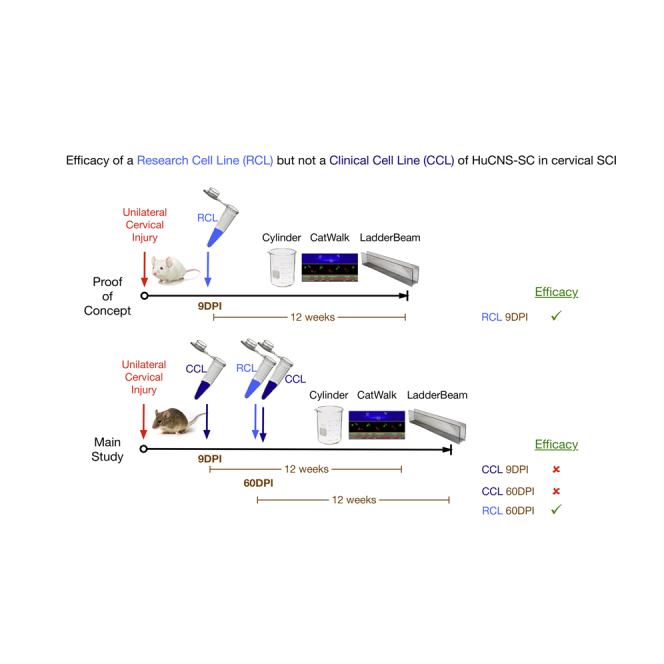
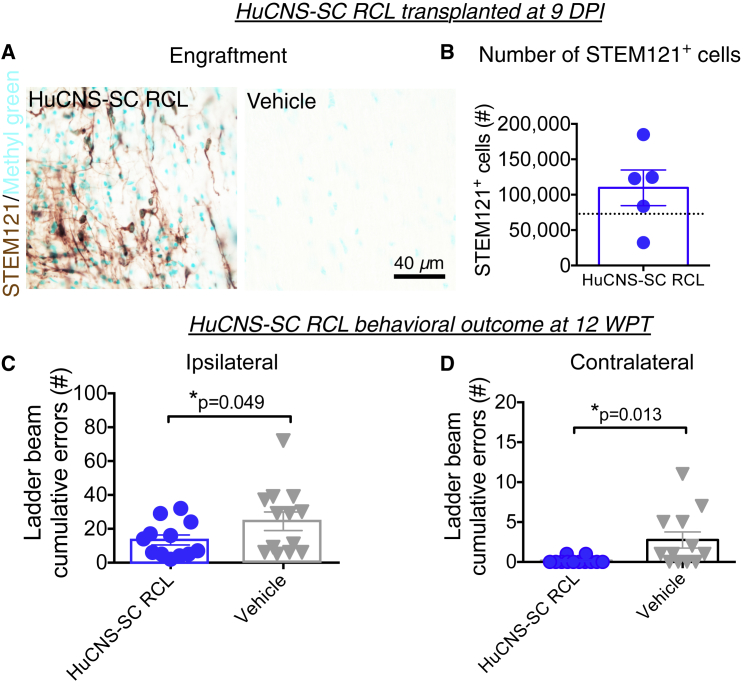
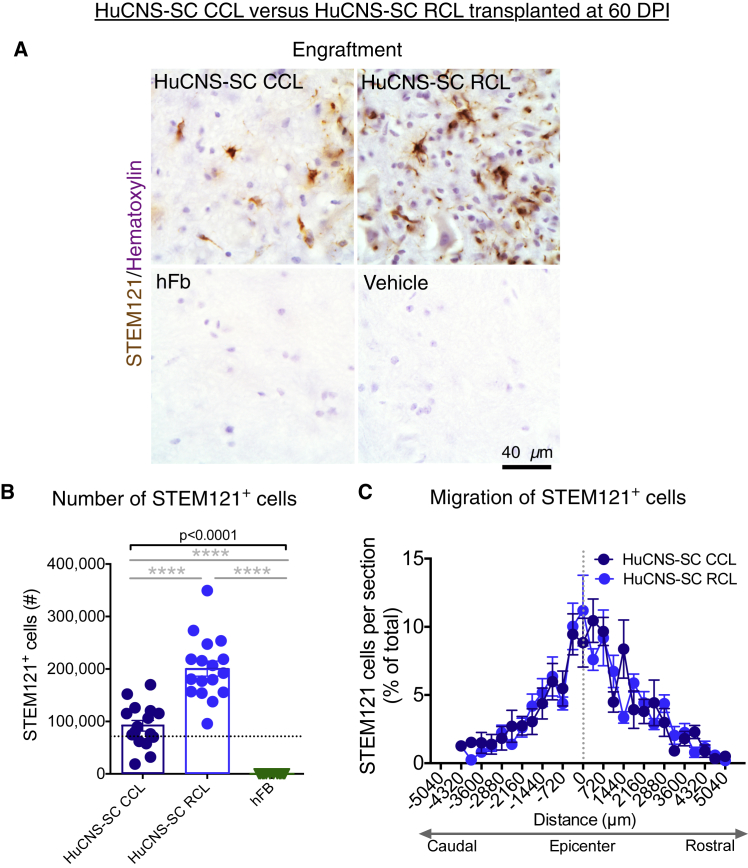
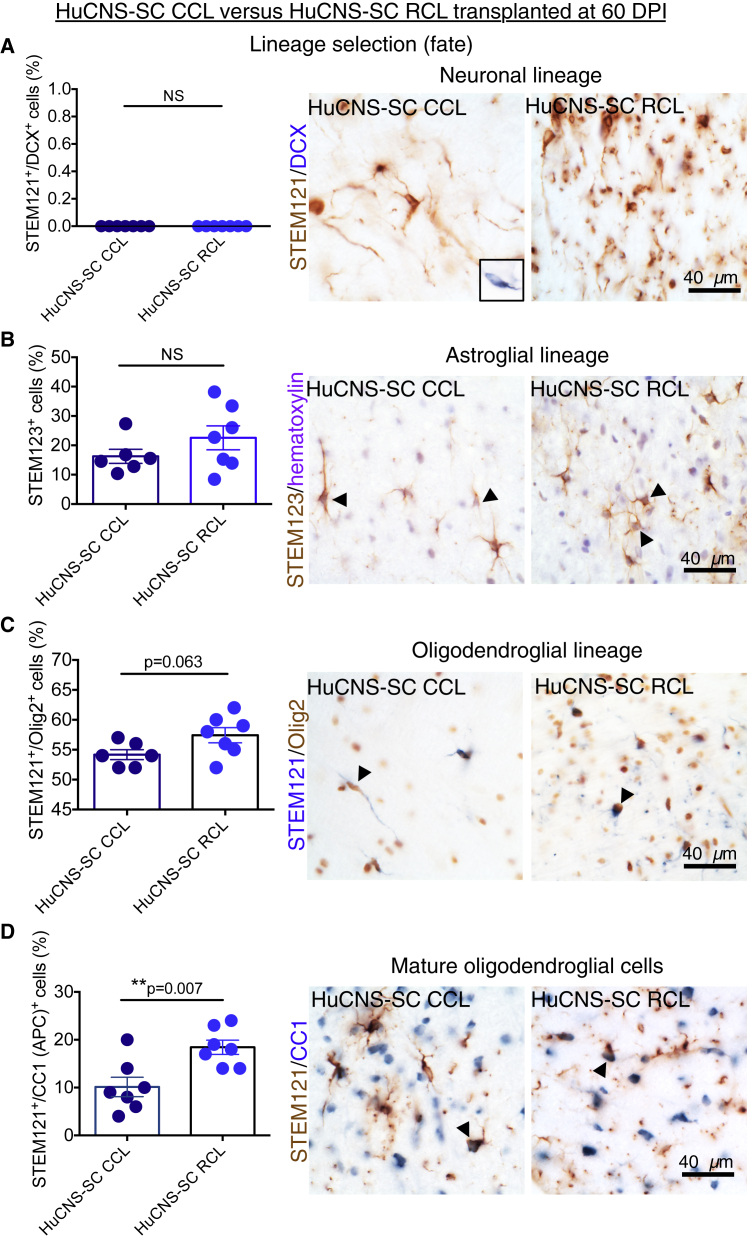
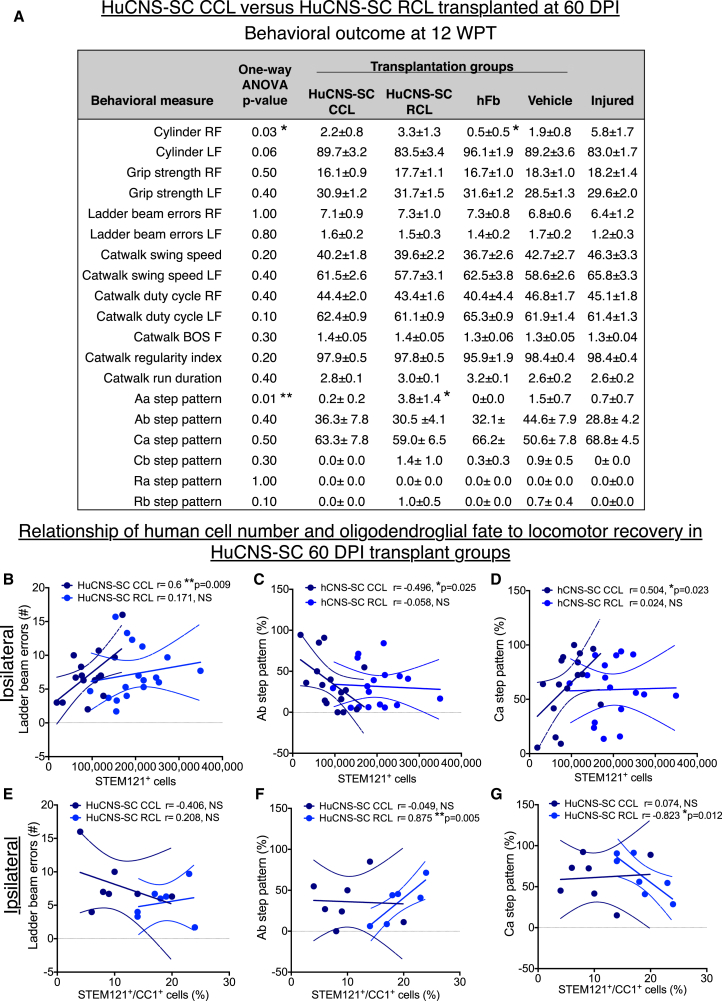
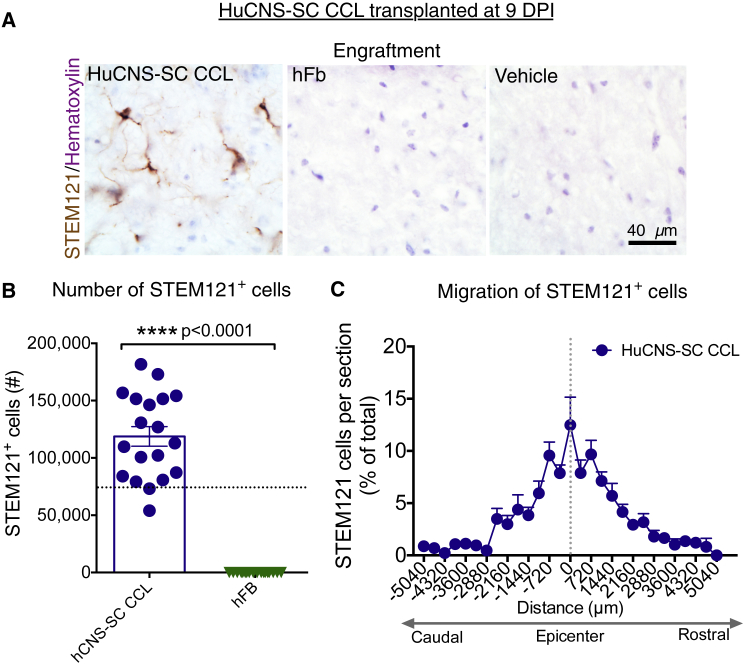
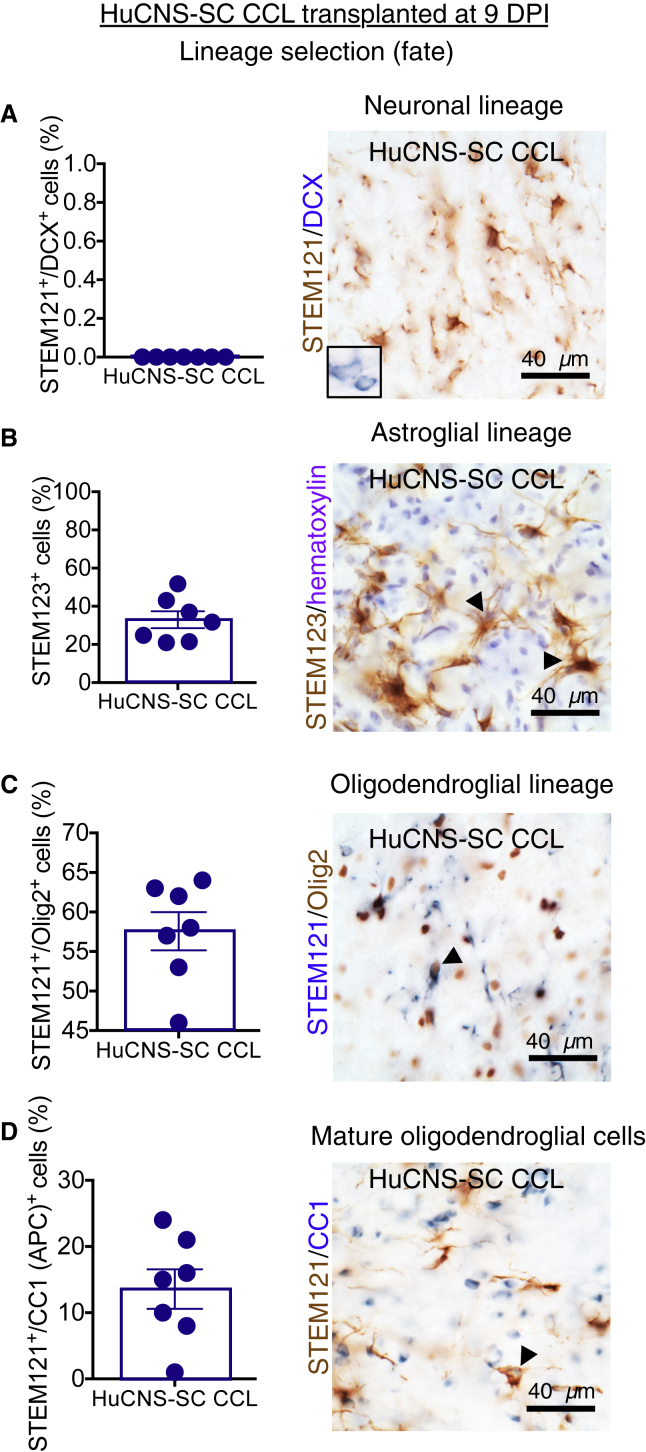
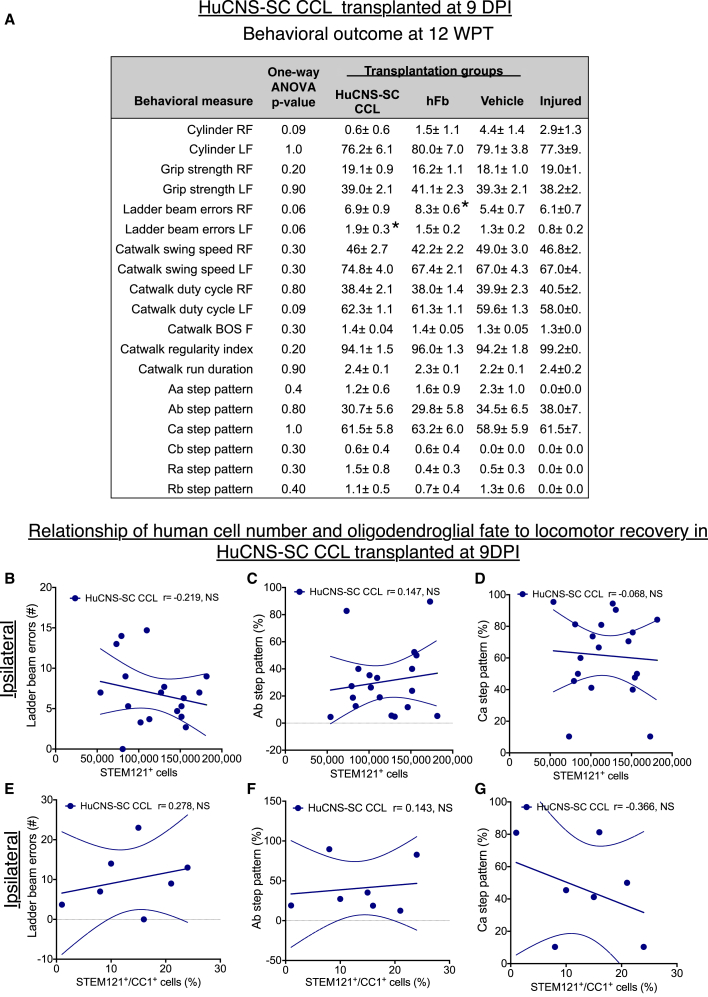
We previously showed the efficacy of multiple research cell lines (RCLs) of human CNS neural stem cells (HuCNS-SCs) in mouse and rat models of thoracic spinal cord injury (SCI), supporting a thoracic SCI clinical trial. Experts recommend in vivo preclinical testing of the intended clinical cell lot/line (CCL) in models with validity for the planned clinical target. We therefore tested the efficacy of two HuCNS-SC lines in cervical SCI: one RCL, and one CCL intended for use in the Pathway Study of cervical SCI in man. We assessed locomotor recovery and sensory function, as well as engraftment, migration, and fate. No evidence of efficacy of the CCL was observed; some data suggested a negative impact of the CCL on outcomes. These data raise questions about the development and validation of potency/comparability assays for clinical testing of cell products, and lack of US Food and Drug Administration requirements for in vivo testing of intended clinical cell lines.
Keywords: FDA guidelines for cell therapies; RIGOR; cervical; efficacy; good manufacturing practices (GMP); human neural stem cells (hNSC); spinal cord injury (SCI).
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Lessons Learned from Pioneering Neural Stem Cell Studies.Stem Cell Reports. 2017 Feb 14;8(2):191-193. doi: 10.1016/j.stemcr.2017.01.024. Stem Cell Reports. 2017. PMID: 28199825 Free PMC article.
-
Response to StemCells Inc.Stem Cell Reports. 2017 Feb 14;8(2):195-197. doi: 10.1016/j.stemcr.2017.02.002. Stem Cell Reports. 2017. PMID: 28199827 Free PMC article. No abstract available.
References
-
- Arvanian V.L., Schnell L., Lou L., Golshani R., Hunanyan A., Ghosh A., Pearse D.D., Robinson J.K., Schwab M.E., Fawcett J.W., Mendell L.M. Chronic spinal hemisection in rats induces a progressive decline in transmission in uninjured fibers to motoneurons. Exp. Neurol. 2009;216:471–480. - PMC - PubMed
-
- Center for Biologics Evaluation and Research . US Department of Health and Huma Services, US Food and Drug Administration and Center for Biologics Evaluation and Research, Office of Communication, Outreach, and Development (OCOD), US Government; 2013. Guidance for Industry - Preclinical Assessment of Investigational Cellular and Gene Therapy Products; p. 35.
-
- Chang J., Phelan M., Cummings B.J. A meta-analysis of efficacy in pre-clinical human stem cell therapies for traumatic brain injury. Exp. Neurol. 2015;273:225–233. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
