

Kinesthetic deficits after perinatal stroke: robotic measurement in hemiparetic children
- PMID: 28202036
- PMCID: PMC5310084
- DOI: 10.1186/s12984-017-0221-6
Kinesthetic deficits after perinatal stroke: robotic measurement in hemiparetic children
Abstract
Background: While sensory dysfunction is common in children with hemiparetic cerebral palsy (CP) secondary to perinatal stroke, it is an understudied contributor to disability with limited objective measurement tools. Robotic technology offers the potential to objectively measure complex sensorimotor function but has been understudied in perinatal stroke. The present study aimed to quantify kinesthetic deficits in hemiparetic children with perinatal stroke and determine their association with clinical function.
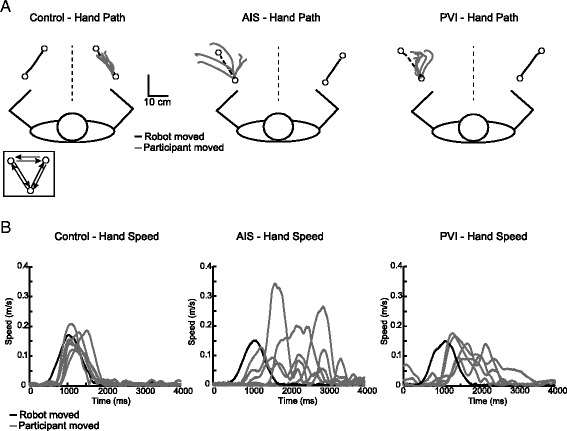
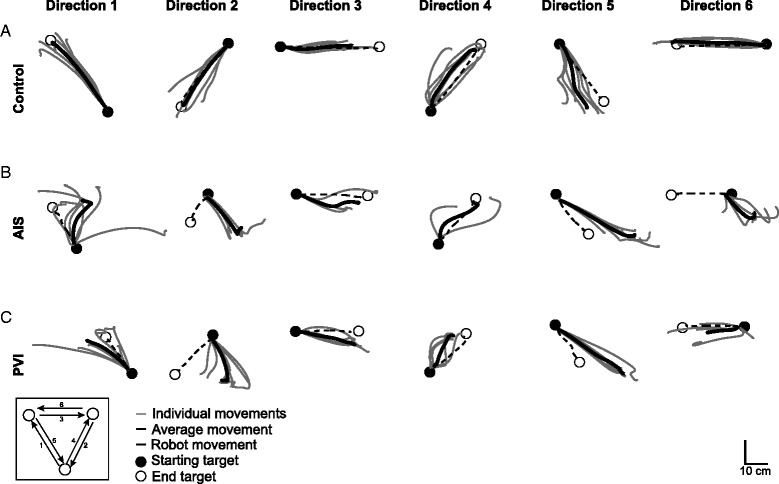
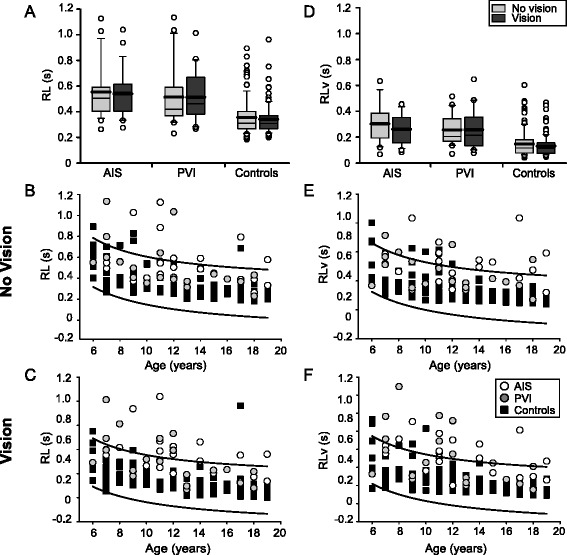
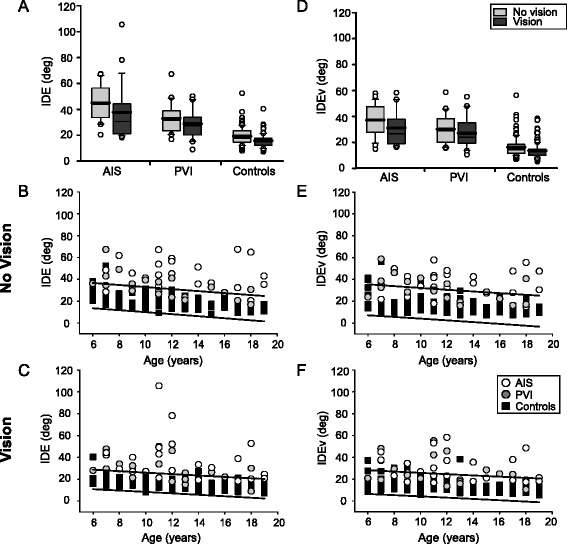
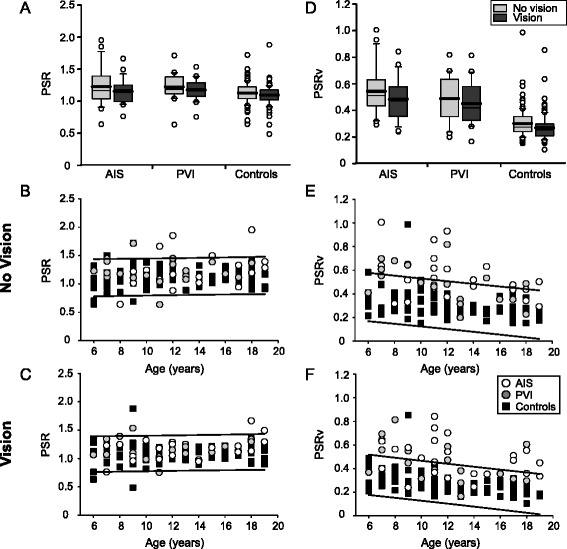
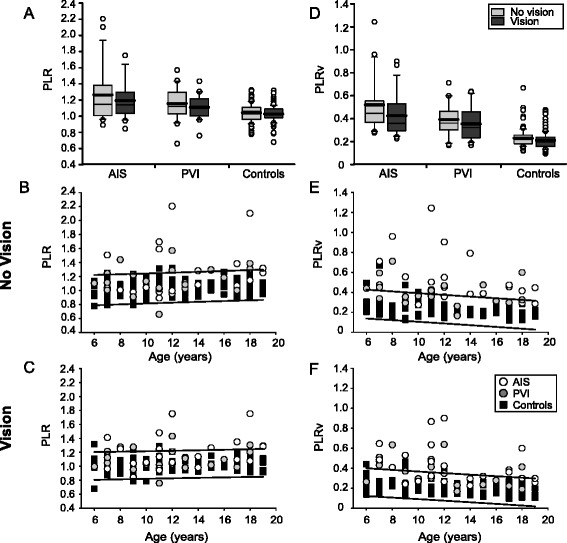
Methods: Case-control study. Participants were 6-19 years of age. Stroke participants had MRI confirmed unilateral perinatal arterial ischemic stroke or periventricular venous infarction, and symptomatic hemiparetic cerebral palsy. Participants completed a robotic assessment of upper extremity kinesthesia using a robotic exoskeleton (KINARM). Four kinesthetic parameters (response latency, initial direction error, peak speed ratio, and path length ratio) and their variabilities were measured with and without vision. Robotic outcomes were compared across stroke groups and controls and to clinical measures of sensorimotor function.
Results: Forty-three stroke participants (23 arterial, 20 venous, median age 12 years, 42% female) were compared to 106 healthy controls. Stroke cases displayed significantly impaired kinesthesia that remained when vision was restored. Kinesthesia was more impaired in arterial versus venous lesions and correlated with clinical measures.
Conclusions: Robotic assessment of kinesthesia is feasible in children with perinatal stroke. Kinesthetic impairment is common and associated with stroke type. Failure to correct with vision suggests sensory network dysfunction.
Keywords: Cerebral palsy; Kinesthesia; Perinatal; Proprioception; Robotics; Stroke.
Figures
References
-
- Sherrington C. On the proprioceptive system, especially in its reflex aspect. Brain. 1907;29:467–82. doi: 10.1093/brain/29.4.467. - DOI
-
- McCloskey DI. Kinesthetic sensibility. Physiol Rev. 1978;58:763–820. - PubMed
-
- Gordon J, Ghilardi MF, Ghez C. Impairments of reaching movements in patients without proprioception. I Spatial errors. J Neurophysiol. 1995;73:347–60. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
