

Isolated IgG4-related sclerosing cholangitis misdiagnosed as malignancy in an area with endemic cholangiocarcinoma: a case report
- PMID: 28202062
- PMCID: PMC5311850
- DOI: 10.1186/s12893-017-0214-1
Isolated IgG4-related sclerosing cholangitis misdiagnosed as malignancy in an area with endemic cholangiocarcinoma: a case report
Abstract
Background: The most common cause of perihilar obstruction is cholangiocarcinoma, especially in Thailand. Benign perihilar stricture represents less than 20% of cases. IgG4-related disease and IgG4-related sclerosing cholangitis, however, have been receiving increased recognition. Isolated IgG4-related sclerosing cholangitis is less common. The preoperative diagnosis of IgG4-related sclerosing cholangitis without pancreatic involvement is very difficult because the clinical presentation and preoperative evaluation are extremely difficult to distinguish from perihilar cholangiocarcinoma.
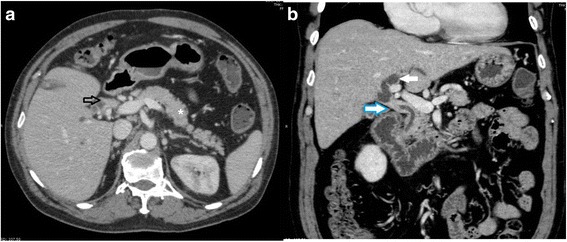
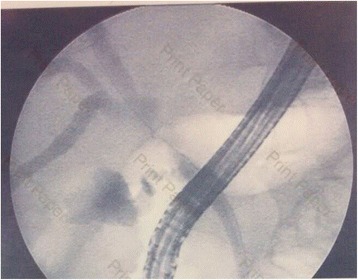
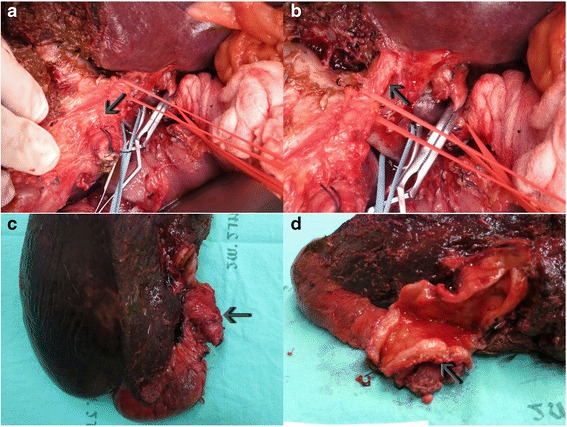
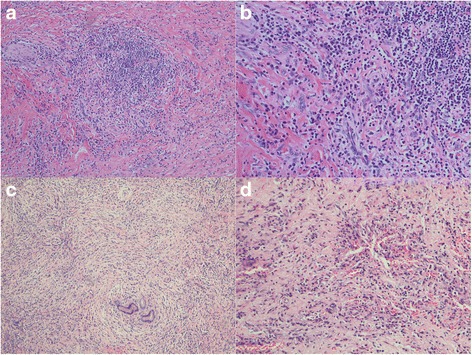
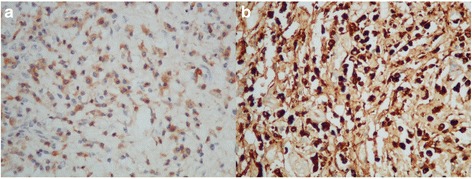
Case presentation: We report the case of a 56-year-old man who presented with obstructive jaundice with preoperative imaging showing proximal common bile duct obstruction. He underwent right lobe liver hepatectomy with extrahepatic bile duct resection and regional lymph node dissection due to high suspicion of malignancy. The pathological report showed severe acute and chronic inflammation of the bile duct with morphology and immunohistochemistry suggestive of IgG4-related sclerosing cholangitis.
Conclusions: IgG4-related sclerosing cholangitis with perihilar obstruction should be considered even in areas where cholangiocarcinoma is endemic.
Keywords: Benign biliary stricture; Cholangiocarcinoma; IgG4, IgG4-related sclerosing cholangitis; Sclerosing cholangitis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
