

MR appearance of the temporal evolution and resolution of spontaneous osteonecrosis of the knee: a case report
- PMID: 28203389
- PMCID: PMC5298408
- DOI: 10.1177/2058460116688719
MR appearance of the temporal evolution and resolution of spontaneous osteonecrosis of the knee: a case report
Abstract
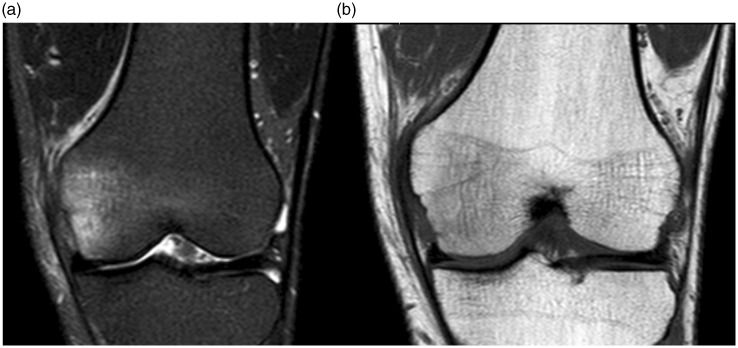
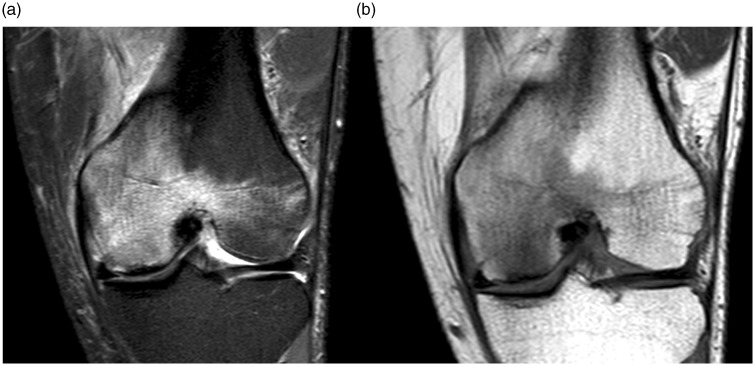
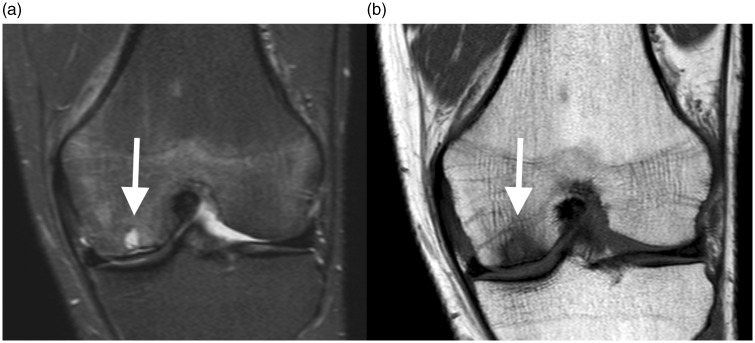
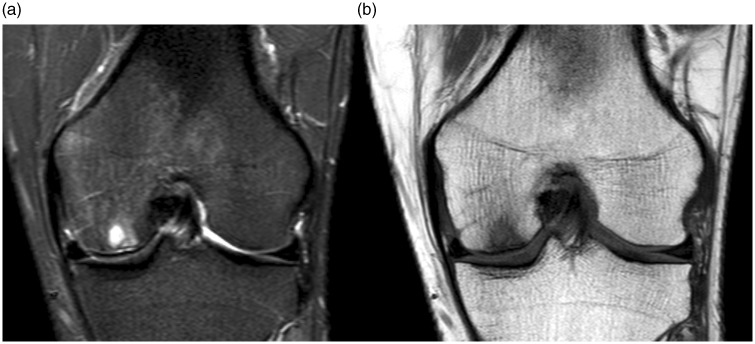
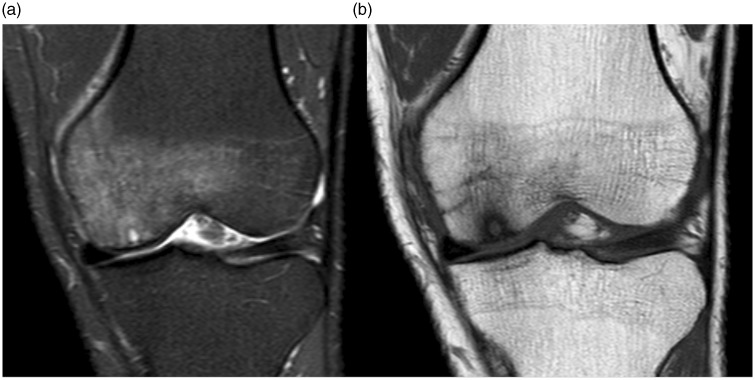
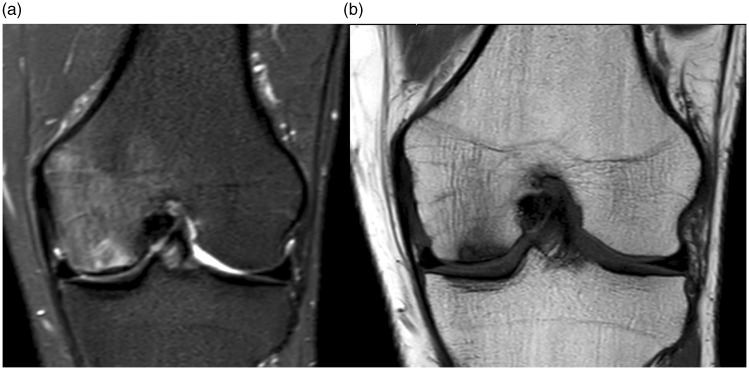
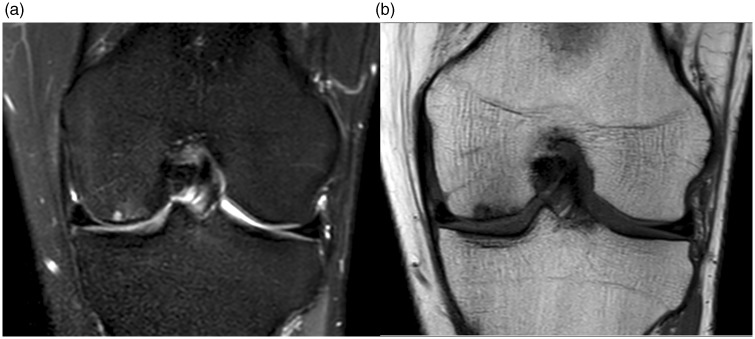
Spontaneous osteonecrosis of the knee (SONK) is a feared condition of unknown cause, in its classic form appearing in the medial femoral condyle in middle-aged or elderly subjects. Diagnosis with radiography is notoriously difficult with a long latency before typical changes appear. Magnetic resonance imaging (MRI) is regarded as a diagnostic tool with the possibility to give an earlier diagnosis with improved chances for treatment. However, also with MRI there may be an initial diagnostic blind spot before typical changes appear. Little is known about the temporal evolution of the MRI changes. In the current case report, a case of SONK is reported where serial imaging with MRI was performed, from initial symptoms to eventual resolution after almost three years.
Keywords: Osteonecrosis; knee; magnetic resonance imaging (MRI).
Figures



References
-
- Bradway JK, Morrey BF. The natural history of the silent hip in bilateral atraumatic osteonecrosis. J Arthroplasty 1993; 8: 383–387. - PubMed
-
- Zywiel MG, McGrath MS, Seyler TM, et al. Osteonecrosis of the knee: a review of three disorders. Orthop Clin North Am 2009; 40: 193–211. - PubMed
-
- Kraenzlin ME, Graf C, Meier C, et al. Possible beneficial effect of bisphosphonates in osteonecrosis of the knee. Knee Surgery, Sport Traumatol Arthrosc 2010; 18: 1638–1644. - PubMed
-
- Kantor H. Bone marrow pressure in osteonecrosis of the femoral condyle (Ahlback’s disease). Arch Orthop Trauma Surg 1987; 106: 349–352. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
