

Incidence of Tuberculosis and Associated Mortality in a Cohort of Human Immunodeficiency Virus-Infected Children Initiating Antiretroviral Therapy
- PMID: 28204517
- PMCID: PMC5907848
- DOI: 10.1093/jpids/piw090
Incidence of Tuberculosis and Associated Mortality in a Cohort of Human Immunodeficiency Virus-Infected Children Initiating Antiretroviral Therapy
Abstract
Background.: We assessed the incidence of tuberculosis, risk factors for tuberculosis, and the contribution of tuberculosis on mortality in a large cohort of human immunodeficiency virus (HIV)-infected children <15 years of age initiating first-line antiretroviral therapy (ART) between 1999 and 2012 in Thailand, one of the 22 high tuberculosis burden countries.
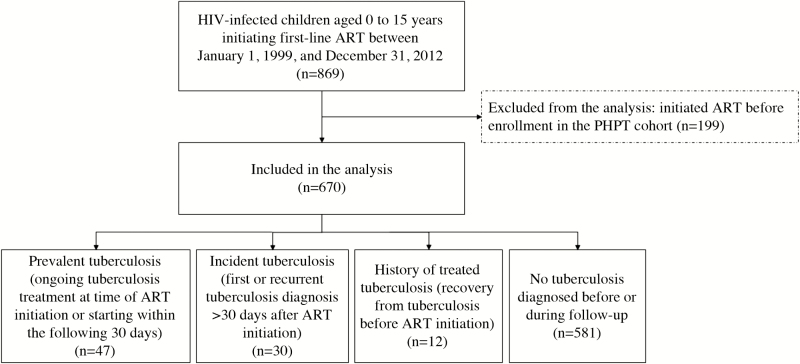
Methods.: A physician reviewed and classified tuberculosis cases. Incidence was the number of children with incident tuberculosis, defined as a first or recurrent tuberculosis diagnosis >30 days after ART initiation, divided by the total person-years of follow-up (PYFU). Risk factors for incident tuberculosis were identified using Fine and Gray's competing risks models, with death from other causes treated as a competing event, and risk factors for death were identified using Cox models.
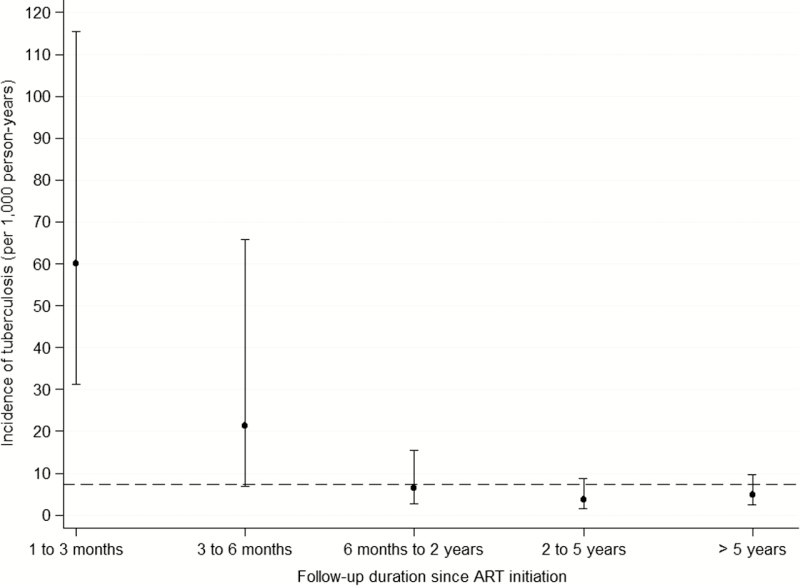
Results.: At ART initiation, 670 children (55% female) had a median age of 6.4 years (interquartile range, 2.0-9.6), body mass index-for-age z-score -0.8 (-1.9 to 0.0), HIV ribonucleic acid viral load 5.1 log10 copies/mL (4.6-5.6), and CD4 9% (3-17). Median duration of follow-up was 7.7 years. Tuberculosis incidence was 7 per 1000 PYFU (95% confidence interval [CI], 5-11) and decreased with ART duration. Lower age-adjusted hemoglobin, hematocrit, and CD4 at ART initiation were associated with a higher risk of incident tuberculosis. Of the 30 incident tuberculosis cases, 9 died. Diagnosis of incident tuberculosis was associated with mortality (unadjusted hazard ratio = 10.2, 95% CI = 4.8-21.5, P < .001 and adjusted hazard ratio = 5.4, 95% CI = 2.5-11.7, P < .001).
Conclusions.: Incident tuberculosis was strongly associated with mortality. CD4 counts or hemoglobin or hematocrit levels may prompt clinicians to consider a possible tuberculosis infection.
Keywords: HIV; children; incidence; mortality; tuberculosis..
© The Author 2017. Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society.
Figures
References
-
- World Health Organization. Global Tuberculosis Report 2015. Geneva: World Health Organization; 2015.
-
- World Health Organization. TB/HIV Facts 2015. Available at: http://www.who.int/hiv/topics/tb/tbhiv_facts_2015/en/ Accessed 5 January 2017.
-
- Thai National AIDS Committee. Thailand AIDS Response Progress Report 2015. Available at: http://www.unaids.org/sites/default/files/country/documents/THA_narrativ... Accessed 5 January 2017.
-
- Nelson LJ, Wells CD. Global epidemiology of childhood tuberculosis. Int J Tuberc Lung Dis 2004; 8:636–47. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
