

Mixed pathologies including chronic traumatic encephalopathy account for dementia in retired association football (soccer) players
- PMID: 28205009
- PMCID: PMC5325836
- DOI: 10.1007/s00401-017-1680-3
Mixed pathologies including chronic traumatic encephalopathy account for dementia in retired association football (soccer) players
Abstract
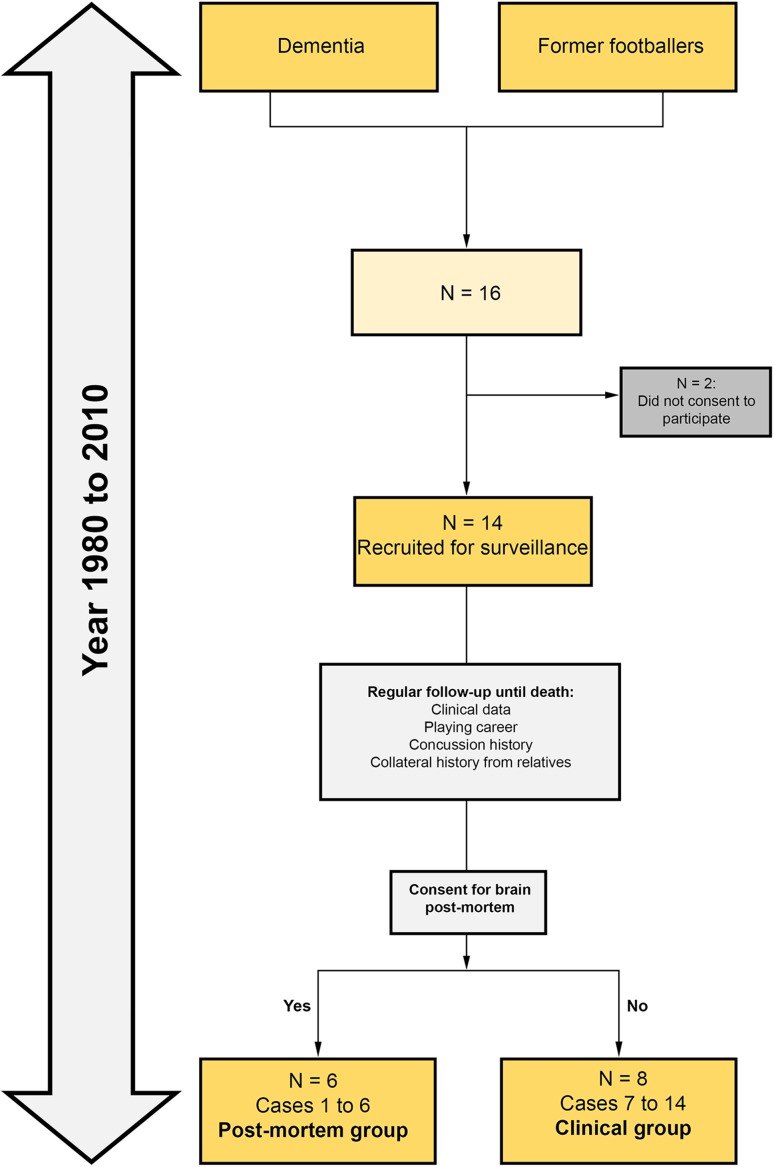
In retired professional association football (soccer) players with a past history of repetitive head impacts, chronic traumatic encephalopathy (CTE) is a potential neurodegenerative cause of dementia and motor impairments. From 1980 to 2010, 14 retired footballers with dementia were followed up regularly until death. Their clinical data, playing career, and concussion history were prospectively collected. Next-of-kin provided consent for six to have post-mortem brain examination. Of the 14 male participants, 13 were professional and 1 was a committed amateur. All were skilled headers of the ball and had played football for an average of 26 years. Concussion rate was limited in six cases to one episode each during their careers. All cases developed progressive cognitive impairment with an average age at onset of 63.6 years and disease duration of 10 years. Neuropathological examination revealed septal abnormalities in all six post-mortem cases, supportive of a history of chronic repetitive head impacts. Four cases had pathologically confirmed CTE; concomitant pathologies included Alzheimer's disease (N = 6), TDP-43 (N = 6), cerebral amyloid angiopathy (N = 5), hippocampal sclerosis (N = 2), corticobasal degeneration (N = 1), dementia with Lewy bodies (N = 1), and vascular pathology (N = 1); and all would have contributed synergistically to the clinical manifestations. The pathological diagnosis of CTE was established in four individuals according to the latest consensus diagnostic criteria. This finding is probably related to their past prolonged exposure to repetitive head impacts from head-to-player collisions and heading the ball thousands of time throughout their careers. Alzheimer's disease and TDP-43 pathologies are common concomitant findings in CTE, both of which are increasingly considered as part of the CTE pathological entity in older individuals. Association football is the most popular sport in the world and the potential link between repetitive head impacts from playing football and CTE as indicated from our findings is of considerable public health interest. Clearly, a definitive link cannot be established in this clinico-pathological series, but our findings support the need for further systematic investigation, including large-scale case-control studies to identify at risk groups of footballers which will justify for the implementation of protective strategies.
Keywords: Chronic traumatic encephalopathy; Concussion; Football; Heading; Soccer; Tauopathy; Traumatic brain injury.
Conflict of interest statement
Funding
The Drake Foundation.
Conflict of interest
The Drake Foundation provided consumable funding for this project. HL and TR are funded by CBD Solutions Research Grant. HRM receives research grants from the Drake Foundation. JWN reports no conflict of interest. JLH is supported by the Multiple System Atrophy Trust, Alzheimer’s Research UK, CBD Solutions, and the Michael J Fox Foundation. Queen Square Brain Bank is supported by Reta Lila Weston Institute for Neurological Studies and the Medical Research Council UK. This research was partly supported by the National Institute for Health Research (NIHR) Queen Square Biomedical Research Unit in Dementia based at University College London Hospitals (UCLH), University College London (UCL). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
Figures
Comment in
-
Traumatic brain injury: New insights into the long-term effects of mild brain injury.Nat Rev Neurol. 2017 Apr;13(4):194-195. doi: 10.1038/nrneurol.2017.32. Epub 2017 Mar 3. Nat Rev Neurol. 2017. PMID: 28257129 No abstract available.
References
-
- Barnes BC, Cooper L, Kirkendall DT, McDermott TP, Jordan BD, Garrett WE., Jr Concussion history in elite male and female soccer players. Am J Sports Med. 1998;26:433–438. - PubMed
-
- Bieniek KF, Ross OA, Cormier KA, Walton RL, Soto-Ortolaza A, Johnston AE, DeSaro P, Boylan KB, Graff-Radford NR, Wszolek ZK, et al. Chronic traumatic encephalopathy pathology in a neurodegenerative disorders brain bank. Acta Neuropathol. 2015;130:877–889. doi: 10.1007/s00401-015-1502-4. - DOI - PMC - PubMed
-
- Boden BP, Kirkendall DT, Garrett WE., Jr Concussion incidence in elite college soccer players. Am J Sports Med. 1998;26:238–241. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
