

Utilizing the Foreign Body Response to Grow Tissue Engineered Blood Vessels in Vivo
- PMID: 28205013
- PMCID: PMC5437130
- DOI: 10.1007/s12265-017-9731-7
Utilizing the Foreign Body Response to Grow Tissue Engineered Blood Vessels in Vivo
Abstract
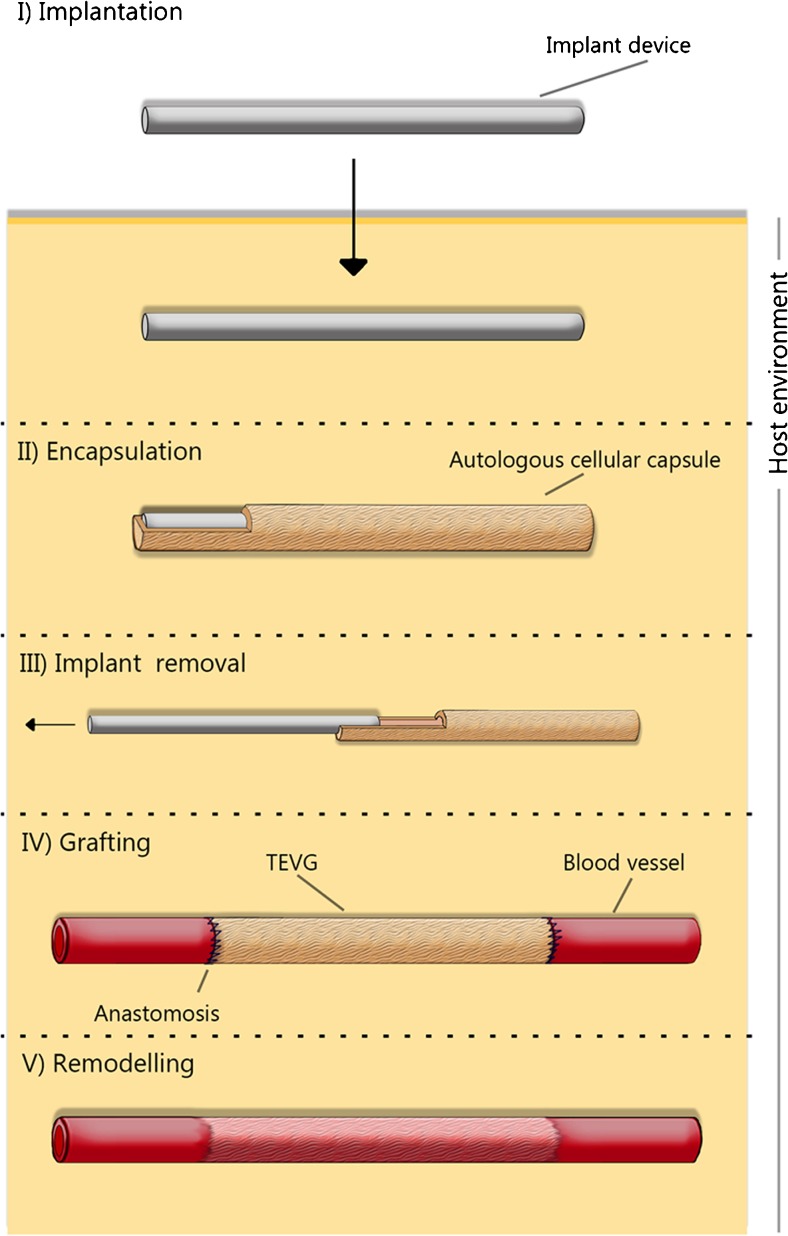
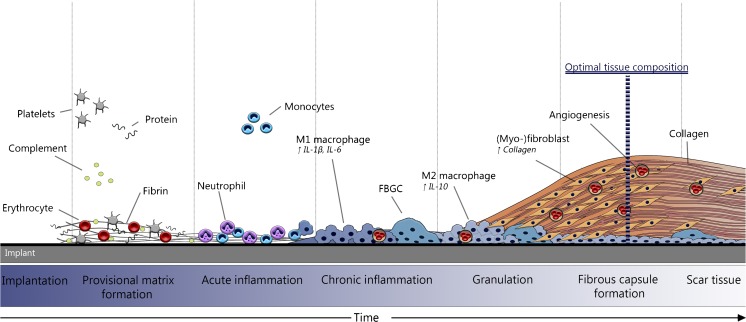
It is well known that the number of patients requiring a vascular grafts for use as vessel replacement in cardiovascular diseases, or as vascular access site for hemodialysis is ever increasing. The development of tissue engineered blood vessels (TEBV's) is a promising method to meet this increasing demand vascular grafts, without having to rely on poorly performing synthetic options such as polytetrafluoroethylene (PTFE) or Dacron. The generation of in vivo TEBV's involves utilizing the host reaction to an implanted biomaterial for the generation of completely autologous tissues. Essentially this approach to the development of TEBV's makes use of the foreign body response to biomaterials for the construction of the entire vascular replacement tissue within the patient's own body. In this review we will discuss the method of developing in vivo TEBV's, and debate the approaches of several research groups that have implemented this method.
Keywords: Animal models; Foreign body response; Graft; Graft patency; In vivo tissue engineering; Tissue engineering; Translational; Vascular access; Vascular graft; Vascular tissue engineering; Vasculature.
Conflict of interest statement
Conflict of Interest
The authors have no conflicts of interest to disclose.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures

Similar articles
-
Tissue engineering of blood vessels in cardiovascular disease: moving towards clinical translation.Heart. 2013 Apr;99(7):454-60. doi: 10.1136/heartjnl-2012-302984. Epub 2013 Jan 30. Heart. 2013. PMID: 23363931 Review.
-
Arterial tissue regeneration for pediatric applications: inspiration from up-to-date tissue-engineered vascular bypass grafts.Artif Organs. 2013 May;37(5):423-34. doi: 10.1111/aor.12022. Epub 2013 Apr 4. Artif Organs. 2013. PMID: 23551257 Review.
-
Combining tissue repair and tissue engineering; bioactivating implantable cell-free vascular scaffolds.Heart. 2014 Dec;100(23):1825-30. doi: 10.1136/heartjnl-2014-306092. Epub 2014 Jul 22. Heart. 2014. PMID: 25053725 Review.
-
In situ tissue regeneration using a novel tissue-engineered, small-caliber vascular graft without cell seeding.J Thorac Cardiovasc Surg. 2008 Oct;136(4):900-7. doi: 10.1016/j.jtcvs.2008.02.058. Epub 2008 Jul 3. J Thorac Cardiovasc Surg. 2008. PMID: 18954628
-
Bioengineered hemodialysis access grafts.J Vasc Access. 2017 Mar 6;18(Suppl. 1):56-63. doi: 10.5301/jva.5000692. Epub 2017 Mar 5. J Vasc Access. 2017. PMID: 28297061 Review.
Cited by
-
Tissue Engineering-Bridging the Gap.J Cardiovasc Transl Res. 2017 Apr;10(2):91-92. doi: 10.1007/s12265-017-9749-x. J Cardiovasc Transl Res. 2017. PMID: 28500574 No abstract available.
-
Progress in the application of patch materials in cardiovascular surgery.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023 Feb 28;48(2):285-293. doi: 10.11817/j.issn.1672-7347.2023.220560. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 36999476 Free PMC article. Chinese, English.
-
Bioengineering Human Tissues and the Future of Vascular Replacement.Circ Res. 2022 Jun 24;131(1):109-126. doi: 10.1161/CIRCRESAHA.121.319984. Epub 2022 Jun 23. Circ Res. 2022. PMID: 35737757 Free PMC article. Review.
-
Arteriovenous access in hemodialysis: A multidisciplinary perspective for future solutions.Int J Artif Organs. 2021 Jan;44(1):3-16. doi: 10.1177/0391398820922231. Epub 2020 May 22. Int J Artif Organs. 2021. PMID: 32438852 Free PMC article. Review.
-
Tissue Engineered Vascular Graft Recipient Interleukin 10 Status Is Critical for Preventing Thrombosis.Adv Healthc Mater. 2020 Dec;9(24):e2001094. doi: 10.1002/adhm.202001094. Epub 2020 Oct 19. Adv Healthc Mater. 2020. PMID: 33073543 Free PMC article.
References
-
- Kainz A, et al. Prediction of prevalence of chronic kidney disease in diabetic patients in countries of the European Union up to 2025. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2015;30(Suppl 4):iv113–iv118. doi: 10.1093/ndt/gfv073. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
