

Missed lung cancer: when, where, and why?
- PMID: 28206951
- PMCID: PMC5338577
- DOI: 10.5152/dir.2016.16187
Missed lung cancer: when, where, and why?
Abstract
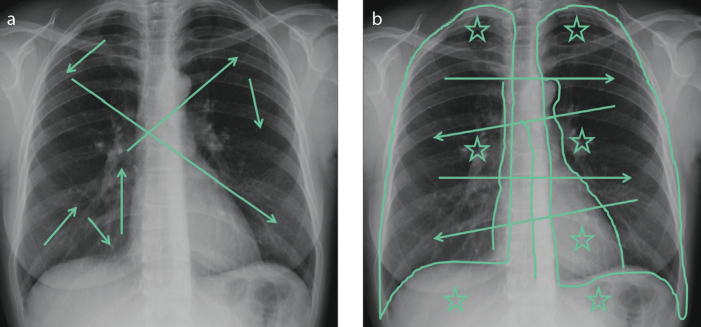
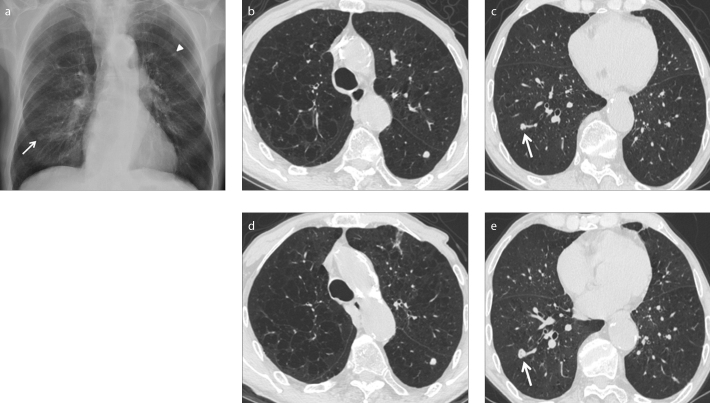
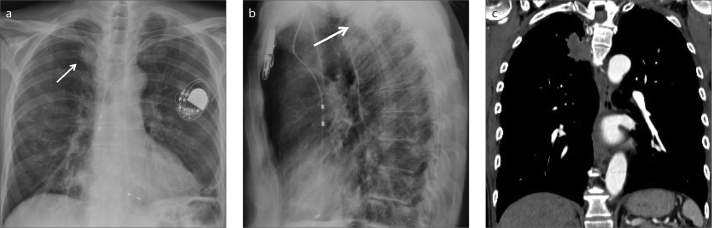
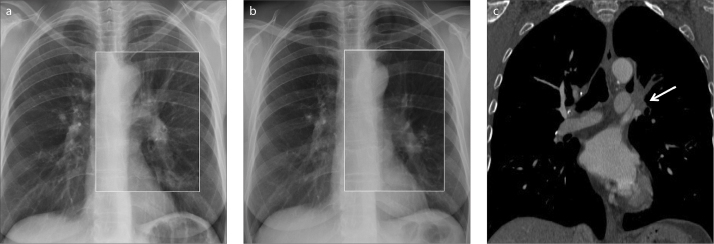
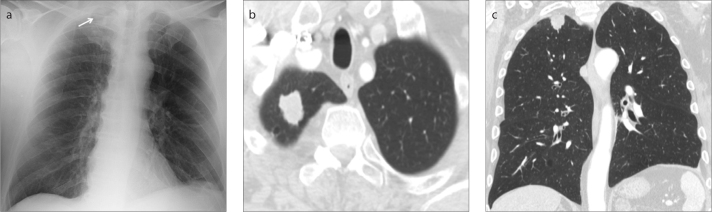
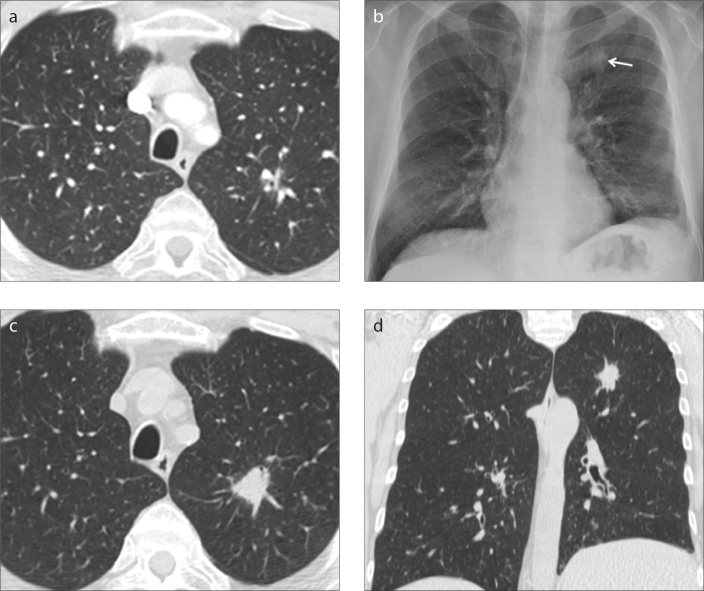
Missed lung cancer is a source of concern among radiologists and an important medicolegal challenge. In 90% of the cases, errors in diagnosis of lung cancer occur on chest radiographs. It may be challenging for radiologists to distinguish a lung lesion from bones, pulmonary vessels, mediastinal structures, and other complex anatomical structures on chest radiographs. Nevertheless, lung cancer can also be overlooked on computed tomography (CT) scans, regardless of the context, either if a clinical or radiologic suspect exists or for other reasons. Awareness of the possible causes of overlooking a pulmonary lesion can give radiologists a chance to reduce the occurrence of this eventuality. Various factors contribute to a misdiagnosis of lung cancer on chest radiographs and on CT, often very similar in nature to each other. Observer error is the most significant one and comprises scanning error, recognition error, decision-making error, and satisfaction of search. Tumor characteristics such as lesion size, conspicuity, and location are also crucial in this context. Even technical aspects can contribute to the probability of skipping lung cancer, including image quality and patient positioning and movement. Albeit it is hard to remove missed lung cancer completely, strategies to reduce observer error and methods to improve technique and automated detection may be valuable in reducing its likelihood.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
-
- World Health Organization. Cancer. Fact Sheet Number 297. [Accessed July 10, 2015]. Available at: www.who.int/mediacentre/factsheets/fs297/en/Last updated July 2015.
-
- Groome PA, Bolejack V, Crowley JJ, et al. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:694–705. https://doi.org/10.1097/JTO.0b013e31812d05d5. - DOI - PubMed
-
- Shah PK, Austin JH, White CS, et al. Missed non-small cell lung cancer: radiographic findings of potentially resectable lesions evident only in retrospect. Radiology. 2003;226:235–241. https://doi.org/10.1148/radiol.2261011924. - DOI - PubMed
-
- White CS, Salis AI, Meyer CA. Missed lung cancer on chest radiography and computed tomography: imaging and medicolegal issue. J Thorac Imaging. 1999;14:63–68. https://doi.org/10.1097/00005382-199901000-00006. - DOI - PubMed
-
- Turkington PM, Kennan N, Greenstone MA. Misinterpretation of the chest x ray as a factor in delayed diagnosis of lung cancer. Postgrad Med J. 2002;78:158–160. https://doi.org/10.1136/pmj.78.917.158. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
