

Intensive Care Unit Admission and Survival among Older Patients with Chronic Obstructive Pulmonary Disease, Heart Failure, or Myocardial Infarction
- PMID: 28208030
- PMCID: PMC5566309
- DOI: 10.1513/AnnalsATS.201611-847OC
Intensive Care Unit Admission and Survival among Older Patients with Chronic Obstructive Pulmonary Disease, Heart Failure, or Myocardial Infarction
Abstract
Rationale: Admission to an intensive care unit (ICU) may be beneficial to patients with pneumonia with uncertain ICU needs; however, evidence regarding the association between ICU admission and mortality for other common conditions is largely unknown.
Objectives: To estimate the relationship between ICU admission and outcomes for hospitalized patients with exacerbation of chronic obstructive pulmonary disease (COPD), exacerbation of heart failure (HF), or acute myocardial infarction (AMI).
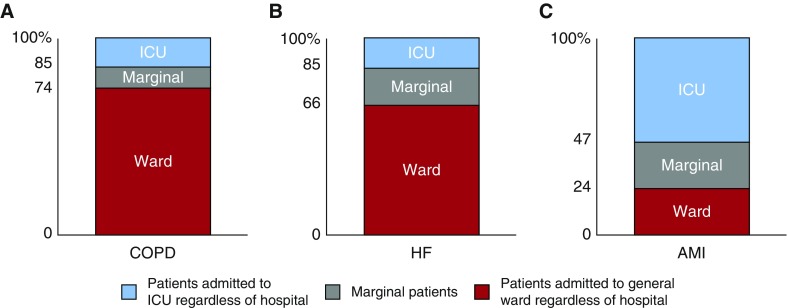
Methods: We performed a retrospective cohort study of all acute care hospitalizations from 2010 to 2012 for U.S. fee-for-service Medicare beneficiaries aged 65 years and older admitted with COPD exacerbation, HF exacerbation, or AMI. We used multivariable adjustment and instrumental variable analysis to assess each condition separately. The instrumental variable analysis used differential distance to a high ICU use hospital (defined separately for each condition) as an instrument for ICU admission to examine marginal patients whose likelihood of ICU admission depended on the hospital to which they were admitted. The primary outcome was 30-day mortality. Secondary outcomes included hospital costs.
Results: Among 1,555,798 Medicare beneficiaries with COPD exacerbation, HF exacerbation, or AMI, 486,272 (31%) were admitted to an ICU. The instrumental variable analysis found that ICU admission was not associated with significant differences in 30-day mortality for any condition. ICU admission was associated with significantly greater hospital costs for HF ($11,793 vs. $9,185, P < 0.001; absolute increase, $2,608 [95% confidence interval, $1,377-$3,840]) and AMI ($19,513 vs. $14,590, P < 0.001; absolute increase, $4,922 [95% confidence interval, $2,665-$7,180]), but not for COPD.
Conclusions: ICU admission did not confer a survival benefit for patients with uncertain ICU needs hospitalized with COPD exacerbation, HF exacerbation, or AMI. These findings suggest that the ICU may be overused for some patients with these conditions. Identifying patients most likely to benefit from ICU admission may improve health care efficiency while reducing costs.
Keywords: chronic obstructive pulmonary disease; heart failure; instrumental variable; intensive care; myocardial infarction.
Figures
Comment in
-
ICUs Overused for Some Elderly Patients.Am J Nurs. 2017 Jun;117(6):70. doi: 10.1097/01.NAJ.0000520259.95577.e3. Am J Nurs. 2017. PMID: 28541995 No abstract available.
-
Canon in Intensive Care Unit Utilization: The Importance of a Fine-Tuned Instrument.Ann Am Thorac Soc. 2017 Jun;14(6):836-838. doi: 10.1513/AnnalsATS.201703-251ED. Ann Am Thorac Soc. 2017. PMID: 28570159 No abstract available.
References
-
- Chang DW, Dacosta D, Shapiro MF. Priority levels in medical intensive care at an academic public hospital. JAMA Intern Med. 2017;177:280–281. - PubMed
-
- Chen LM, Render M, Sales A, Kennedy EH, Wiitala W, Hofer TP. Intensive care unit admitting patterns in the Veterans Affairs health care system. Arch Intern Med. 2012;172:1220–1226. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
