

Lingual Tonsillectomy for Treatment of Pediatric Obstructive Sleep Apnea: A Meta-analysis
- PMID: 28208178
- PMCID: PMC5824231
- DOI: 10.1001/jamaoto.2016.4274
Lingual Tonsillectomy for Treatment of Pediatric Obstructive Sleep Apnea: A Meta-analysis
Abstract
Importance: Evidence indicates correlations between lingual tonsil hypertrophy and pediatric obstructive sleep apnea (OSA). However, to our knowledge, a meta-analysis of surgical outcomes for lingual tonsillectomy in children with OSA has not been conducted.
Objective: To evaluate the therapeutic outcomes of lingual tonsillectomy for treatment of pediatric OSA.
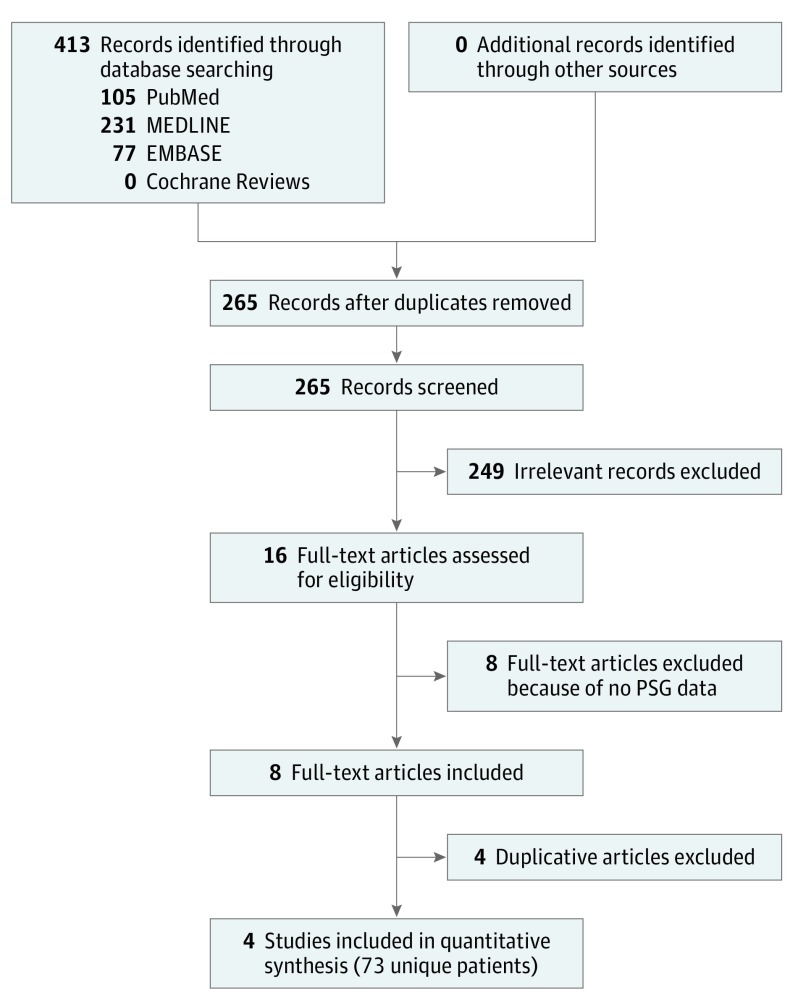
Data sources: The study protocol was registered on PROSPERO (CRD42015027053). PubMed, MEDLINE, EMBASE, and the Cochrane Reviews databases were searched independently by 2 authors for relevant articles published by September 2016.
Study selection: The literature search identified English-language studies that used polysomnography to evaluate children with lingual tonsil hypertrophy and OSA after lingual tonsillectomy alone. The search keywords were lingual tonsil, lingual tonsillectomy, sleep endoscopy, sleep apnea, and child.
Data extraction and synthesis: Polysomnographic data from each study were extracted. A random-effects model pooled postoperative sleep variable changes and success rates for lingual tonsillectomy in treating pediatric OSA.
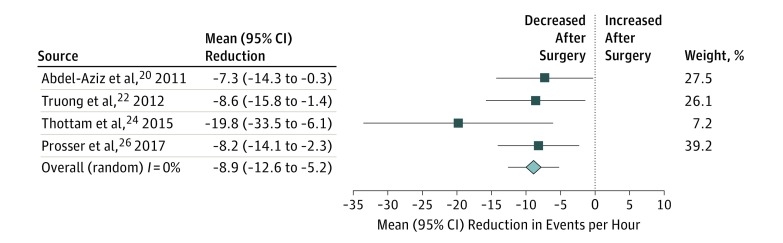
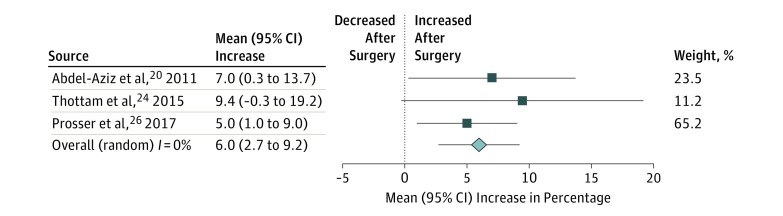
Main outcomes and measures: Four outcomes for lingual tonsillectomy were analyzed. These included net postoperative changes in the apnea-hypopnea index (AHI), net postoperative changes in the minimum oxygen saturation, the overall success rate for a postoperative AHI less than 1, and the overall success rate for a postoperative AHI less than 5.
Results: This meta-analysis consisted of 4 studies (mean sample size, 18.25 patients), with a total of 73 unique patients (mean [SD] age, 8.3 [1.1] years). Fifty-nine percent (27 of 46) of the patients were male, and 1 of the 4 studies did not specify number of males. Lingual tonsillectomy was indicated for persistent OSA after adenotonsillectomy in all cases. Lingual tonsil hypertrophy was evaluated using computed tomography or magnetic resonance imaging in 1 study, sleep endoscopy in 2 studies, and cine magnetic resonance imaging in 1 study. The mean change in the AHI after lingual tonsillectomy was a reduction of 8.9 (95% CI, -12.6 to -5.2) events per hour. The mean change in the minimum oxygen saturation after lingual tonsillectomy was an increase of 6.0% (95% CI, 2.7%-9.2%). The overall success rate was 17% (95% CI, 7%-35%) for a postoperative AHI less than 1 and 51% (95% CI, 25%-76%) for a postoperative AHI less than 5. Postoperative complications that developed included airway obstruction, bleeding, and pneumonia.
Conclusions and relevance: Lingual tonsillectomy is an effective surgical management for children with OSA caused by lingual tonsil hypertrophy, and it achieves significant improvement in the AHI and the minimum oxygen saturation. However, children frequently have residual OSA after lingual tonsillectomy, and postoperative complications must be carefully managed.
Conflict of interest statement
Figures
References
-
- Marcus CL, Brooks LJ, Draper KA, et al. ; American Academy of Pediatrics . Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):576-584. - PubMed
-
- Kang KT, Lee PL, Weng WC, Hsu WC. Body weight status and obstructive sleep apnea in children. Int J Obes (Lond). 2012;36(7):920-924. - PubMed
-
- Nolan J, Brietzke SE. Systematic review of pediatric tonsil size and polysomnogram-measured obstructive sleep apnea severity. Otolaryngol Head Neck Surg. 2011;144(6):844-850. - PubMed
-
- Kang KT, Weng WC, Lee CH, Hsiao TY, Lee PL, Hsu WC. Clinical risk assessment model for pediatric obstructive sleep apnea. Laryngoscope. 2016;126(10):2403-2409. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
