

Pathogenesis and Therapeutic Mechanisms in Immune Thrombocytopenia (ITP)
- PMID: 28208757
- PMCID: PMC5332920
- DOI: 10.3390/jcm6020016
Pathogenesis and Therapeutic Mechanisms in Immune Thrombocytopenia (ITP)
Abstract
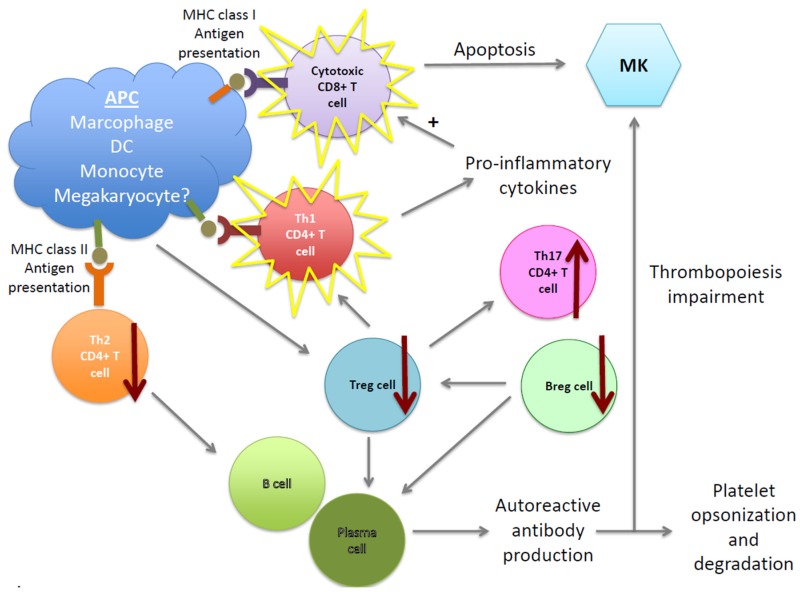
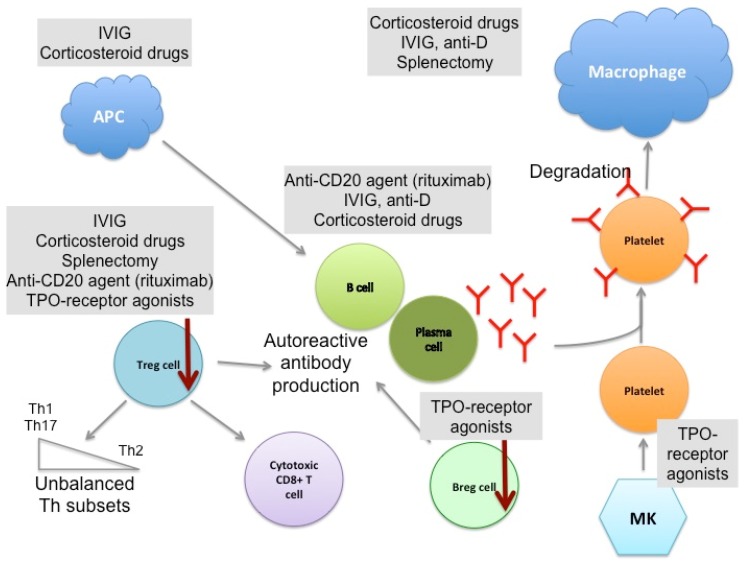
Immune thrombocytopenia (ITP) is a complex autoimmune disease characterized by low platelet counts. The pathogenesis of ITP remains unclear although both antibody-mediated and/or T cell-mediated platelet destruction are key processes. In addition, impairment of T cells, cytokine imbalances, and the contribution of the bone marrow niche have now been recognized to be important. Treatment strategies are aimed at the restoration of platelet counts compatible with adequate hemostasis rather than achieving physiological platelet counts. The first line treatments focus on the inhibition of autoantibody production and platelet degradation, whereas second-line treatments include immunosuppressive drugs, such as Rituximab, and splenectomy. Finally, thirdline treatments aim to stimulate platelet production by megakaryocytes. This review discusses the pathophysiology of ITP and how the different treatment modalities affect the pathogenic mechanisms.
Keywords: immune thrombocytopenia (ITP); B cells; T cells; autoimmunity; platelets.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Rodeghiero F., Stasi R., Gernsheimer T., Michel M., Provan D., Arnold D.M., Bussel J.B., Cines D.B., Chong B.H., Cooper N., et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from an international working group. Blood. 2009;113:2386–2393. doi: 10.1182/blood-2008-07-162503. - DOI - PubMed
-
- Harrington W.J., Minnich V., Hollingsworth J.W., Moore C.V. Demonstration of a thrombocytopenic factor in the blood of patients with thrombocytopenic purpura. J. Lab. Clin. Med. 1951;38:1–10. - PubMed
-
- Shulman N.R., Marder V.J., Weinrach R.S. Similarities between known antiplatelet antibodies and the factor responsible for thrombocytopenia in idiopathic purpura. Physiologic, serologic and isotopic studies. Ann. N. Y. Acad. Sci. 1965;124:499–542. doi: 10.1111/j.1749-6632.1965.tb18984.x. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
