

Best time to assess complete clinical response after chemoradiotherapy in squamous cell carcinoma of the anus (ACT II): a post-hoc analysis of randomised controlled phase 3 trial
- PMID: 28209296
- PMCID: PMC5337624
- DOI: 10.1016/S1470-2045(17)30071-2
Best time to assess complete clinical response after chemoradiotherapy in squamous cell carcinoma of the anus (ACT II): a post-hoc analysis of randomised controlled phase 3 trial
Erratum in
-
Correction to Lancet Oncol 2017; 18: 347-56.Lancet Oncol. 2017 Apr;18(4):e196. doi: 10.1016/S1470-2045(17)30173-0. Epub 2017 Mar 3. Lancet Oncol. 2017. PMID: 28262462 Free PMC article. No abstract available.
-
Correction to Lancet Oncol 2017; 18: 347-56.Lancet Oncol. 2020 Nov;21(11):e518. doi: 10.1016/S1470-2045(20)30583-0. Lancet Oncol. 2020. PMID: 33152308 No abstract available.
Abstract
Background: Guidelines for anal cancer recommend assessment of response at 6-12 weeks after starting treatment. Using data from the ACT II trial, we determined the optimum timepoint to assess clinical tumour response after chemoradiotherapy.
Methods: The previously reported ACT II trial was a phase 3 randomised trial of patients of any age with newly diagnosed, histologically confirmed, squamous cell carcinoma of the anus without metastatic disease from 59 centres in the UK. We randomly assigned patients (by minimisation) to receive either intravenous mitomycin (one dose of 12 mg/m2 on day 1) or intravenous cisplatin (one dose of 60 mg/m2 on days 1 and 29), with intravenous fluorouracil (one dose of 1000 mg/m2 per day on days 1-4 and 29-32) and radiotherapy (50·4 Gy in 28 daily fractions); and also did a second randomisation after initial therapy to maintenance chemotherapy (fluorouracil and cisplatin) or no maintenance chemotherapy. The primary outcome was complete clinical response (the absence of primary and nodal tumour by clinical examination), in addition to overall survival and progression-free survival from time of randomisation. In this post-hoc analysis, we analysed complete clinical response at three timepoints: 11 weeks from the start of chemoradiotherapy (assessment 1), 18 weeks from the start of chemoradiotherapy (assessment 2), and 26 weeks from the start of chemoradiotherapy (assessment 3) as well as the overall and progression-free survival estimates of patients with complete clinical response or without complete clinical response at each assessment. We analysed both the overall trial population and a subgroup of patients who had attended each of the three assessments by modified intention-to-treat. This study is registered at controlled-trials.com, ISRCTN 26715889.
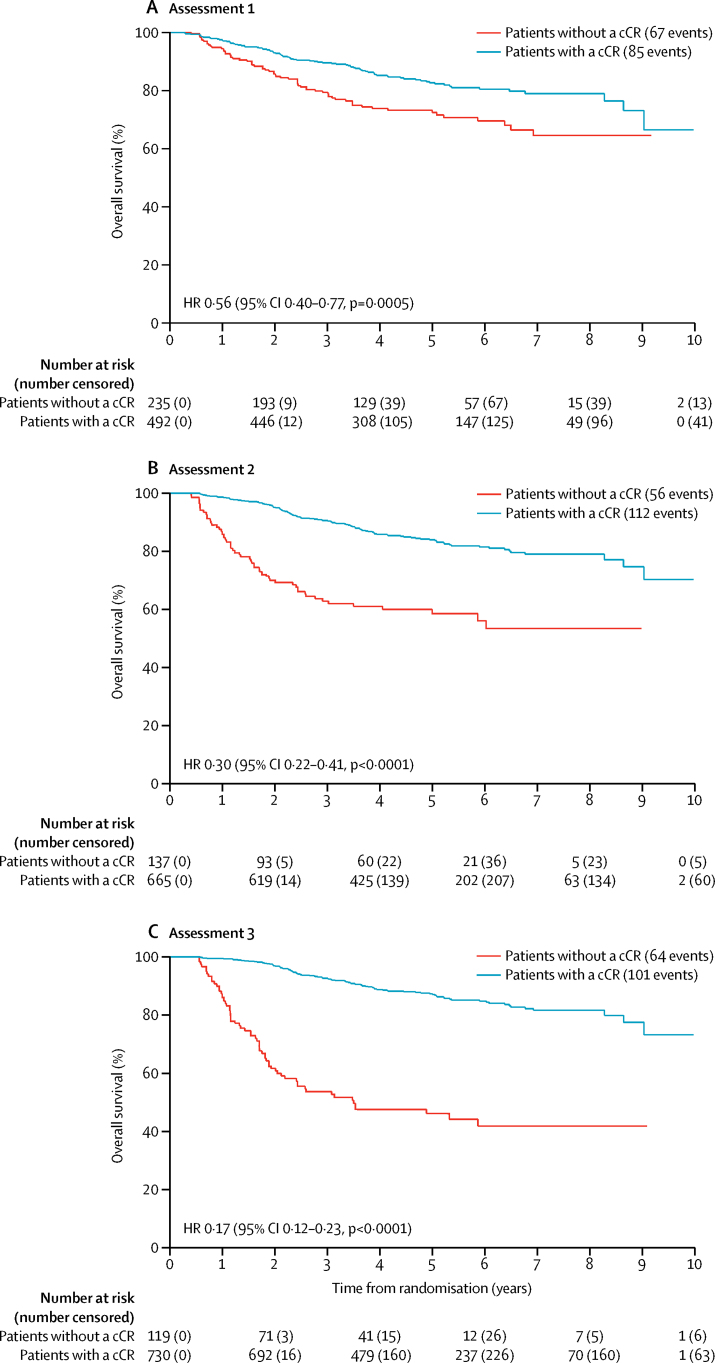
Findings: We enrolled 940 patients from June 4, 2001, until Dec 16, 2008. Complete clinical response was achieved in 492 (52%) of 940 patients at assessment 1 (11 weeks), 665 (71%) of patients at assessment 2 (18 weeks), and 730 (78%) of patients at assessment 3 (26 weeks). 691 patients attended all three assessments and in this subgroup, complete clinical response was reported in 441 (64%) patients at assessment 1, 556 (80%) at assessment 2, and 590 (85%) at assessments 3. 151 (72%) of the 209 patients who had not had a complete clinical response at assessment 1 had a complete clinical response by assessment 3. In the overall trial population of 940 patients, 5 year overall survival in patients who had a clinical response at assessments 1, 2, 3 was 83% (95% CI 79-86), 84% (81-87), and 87% (84-89), respectively and was 72% (66-78), 59% (49-67), and 46% (37-55) for patients who did not have a complete clinical response at assessments 1, 2, 3, respectively. In the subgroup of 691 patients, 5 year overall survival in patients who had a clinical response at assessment 1, 2, 3 was 85% (81-88), 86% (82-88), and 87% (84-90), respectively, and was 75% (68-80), 61% (50-70), and 48% (36-58) for patients who did not have a complete clinical response at assessment 1, 2, 3, respectively. Similarly, progression-free survival in both the overall trial population and the subgroup was longer in patients who had a complete clinical response, compared with patients who did not have a complete clinical response, at all three assessments.
Interpretation: Many patients who do not have a complete clinical response when assessed at 11 weeks after commencing chemoradiotherapy do in fact respond by 26 weeks, and the earlier assessment could lead to some patients having unnecessary surgery. Our data suggests that the optimum time for assessment of complete clinical response after chemoradiotherapy for patients with squamous cell carcinoma of the anus is 26 weeks from starting chemoradiotherapy. We suggest that guidelines should be revised to indicate that later assessment is acceptable.
Funding: Cancer Research UK.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures


Comment in
-
Anal cancer: leading the way.Lancet Oncol. 2017 Mar;18(3):276-277. doi: 10.1016/S1470-2045(17)30073-6. Epub 2017 Feb 11. Lancet Oncol. 2017. PMID: 28209297 No abstract available.
-
[How long should we wait upon completion of chemoradiotherapy before assessment of tumor response in anal cancer?].Strahlenther Onkol. 2017 Jul;193(7):593-594. doi: 10.1007/s00066-017-1149-2. Strahlenther Onkol. 2017. PMID: 28523338 German. No abstract available.
-
Gastrointestinal Cancers: Timing Is Everything.Int J Radiat Oncol Biol Phys. 2017 Dec 1;99(5):1051-1058. doi: 10.1016/j.ijrobp.2017.05.040. Int J Radiat Oncol Biol Phys. 2017. PMID: 29165271 Free PMC article. No abstract available.
References
-
- Flam M, John M, Pajak TF. Role of mitomycin in combination with fluorouracil and radiotherapy and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J Clin Oncol. 1996;14:2527–2539. - PubMed
-
- UKCCCR Anal Cancer Working Party: epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil and mitomycin. Lancet. 1996;348:1049–1054. - PubMed
-
- Bartelink H, Roelofsen F, Eschwege F. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J Clin Oncol. 1997;15:2040–2049. - PubMed
-
- Ajani JA, Winter KA, Gunderson LL. Fluorouracil, mitomycin and radiotherapy vs fluorouracil, cisplatin and radiotherapy for carcinoma of the anal canal: a randomised controlled trial. JAMA. 2008;199:1914–1921. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
