

Readiness for Delivering Digital Health at Scale: Lessons From a Longitudinal Qualitative Evaluation of a National Digital Health Innovation Program in the United Kingdom
- PMID: 28209558
- PMCID: PMC5334516
- DOI: 10.2196/jmir.6900
Readiness for Delivering Digital Health at Scale: Lessons From a Longitudinal Qualitative Evaluation of a National Digital Health Innovation Program in the United Kingdom
Abstract
Background: Digital health has the potential to support care delivery for chronic illness. Despite positive evidence from localized implementations, new technologies have proven slow to become accepted, integrated, and routinized at scale.
Objective: The aim of our study was to examine barriers and facilitators to implementation of digital health at scale through the evaluation of a £37m national digital health program: ‟Delivering Assisted Living Lifestyles at Scale" (dallas) from 2012-2015.
Methods: The study was a longitudinal qualitative, multi-stakeholder, implementation study. The methods included interviews (n=125) with key implementers, focus groups with consumers and patients (n=7), project meetings (n=12), field work or observation in the communities (n=16), health professional survey responses (n=48), and cross program documentary evidence on implementation (n=215). We used a sociological theory called normalization process theory (NPT) and a longitudinal (3 years) qualitative framework analysis approach. This work did not study a single intervention or population. Instead, we evaluated the processes (of designing and delivering digital health), and our outcomes were the identified barriers and facilitators to delivering and mainstreaming services and products within the mixed sector digital health ecosystem.
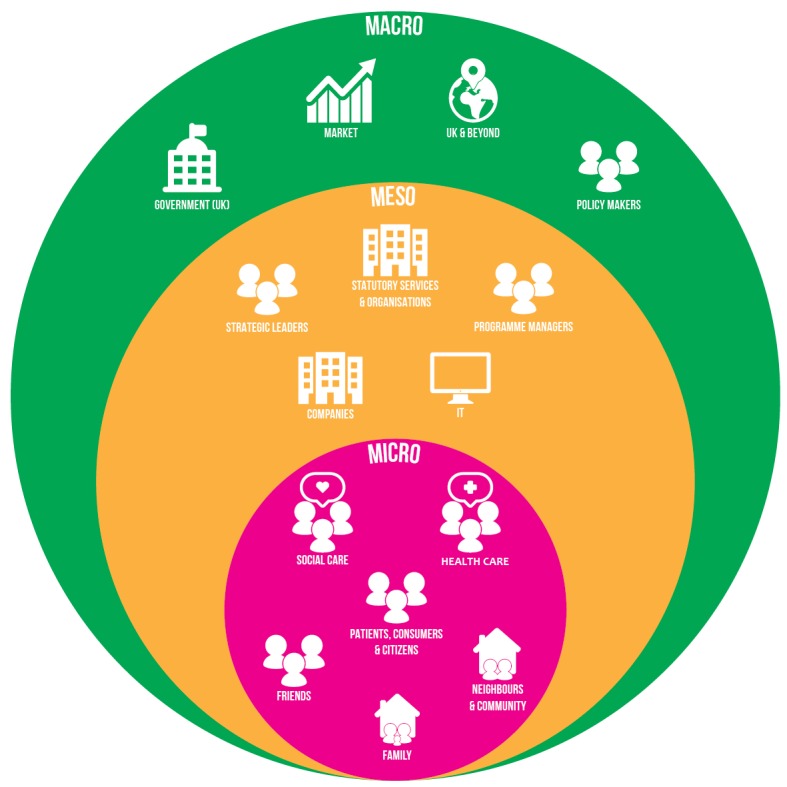
Results: We identified three main levels of issues influencing readiness for digital health: macro (market, infrastructure, policy), meso (organizational), and micro (professional or public). Factors hindering implementation included: lack of information technology (IT) infrastructure, uncertainty around information governance, lack of incentives to prioritize interoperability, lack of precedence on accountability within the commercial sector, and a market perceived as difficult to navigate. Factors enabling implementation were: clinical endorsement, champions who promoted digital health, and public and professional willingness.
Conclusions: Although there is receptiveness to digital health, barriers to mainstreaming remain. Our findings suggest greater investment in national and local infrastructure, implementation of guidelines for the safe and transparent use and assessment of digital health, incentivization of interoperability, and investment in upskilling of professionals and the public would help support the normalization of digital health. These findings will enable researchers, health care practitioners, and policy makers to understand the current landscape and the actions required in order to prepare the market and accelerate uptake, and use of digital health and wellness services in context and at scale.
Keywords: community health services; diffusion of innovation; electronic health records; health plan implementation; health services research; instrumentation; medical informatics; qualitative research; telemedicine.
©Marilyn R Lennon, Matt-Mouley Bouamrane, Alison M Devlin, Siobhan O'Connor, Catherine O'Donnell, Ula Chetty, Ruth Agbakoba, Annemieke Bikker, Eleanor Grieve, Tracy Finch, Nicholas Watson, Sally Wyke, Frances S Mair. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 16.02.2017.
Conflict of interest statement
Conflicts of Interest: All authors have declared that they (1) have support from University of Glasgow, University of Strathclyde, University of Newcastle and Innovate UK for the submitted work, (2) have no relationships with any companies that have an interest in the submitted work in the previous 3 years, (3) their spouses, partners, or children have no financial relationships relevant to the submitted work, and (4) have no other nonfinancial interests that may be relevant to the submitted work.
Figures
References
-
- Jennett PA, Andruchuk K. Telehealth: 'real life' implementation issues. Comput Methods Programs Biomed. 2001 Mar;64(3):169–74.S016926070000136X - PubMed
-
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581–629. doi: 10.1111/j.0887-378X.2004.00325.x. http://europepmc.org/abstract/MED/15595944 MILQ325 - DOI - PMC - PubMed
-
- Mair F, May C, O'Donnell C, Finch T, Sullivan F, Murray E. Factors that promote or inhibit the implementation of e-health systems: an explanatory systematic review. Bull World Health Organ. 2012 May 01;90(5):357–64. doi: 10.2471/BLT.11.099424. http://www.scielosp.org/scielo.php?script=sci_arttext&pid=BLT.11.099424&... BLT.11.099424 - DOI - PMC - PubMed
-
- Bowes A, McColgan G. Implementing telecare for people with dementia: supporting ageing in place in West Lothian, Scotland. J Care Serv Manag. 2013 Jul 18;3(3):227–243. doi: 10.1179/csm.2009.3.3.227. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
