

A Randomized Crossover Trial of Dietary Sodium Restriction in Stage 3-4 CKD
- PMID: 28209636
- PMCID: PMC5338699
- DOI: 10.2215/CJN.01120216
A Randomized Crossover Trial of Dietary Sodium Restriction in Stage 3-4 CKD
Abstract
Background and objectives: Patients with chronic kidney disease (CKD) are often volume expanded and hypertensive. Few controlled studies have assessed the effects of a sodium-restricted diet (SRD) in CKD.
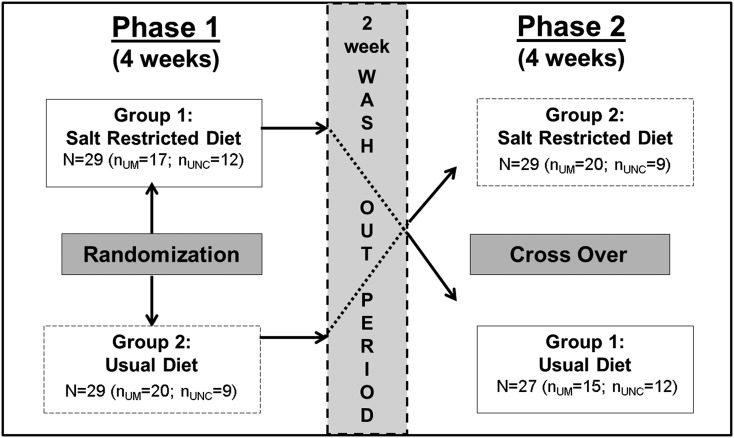
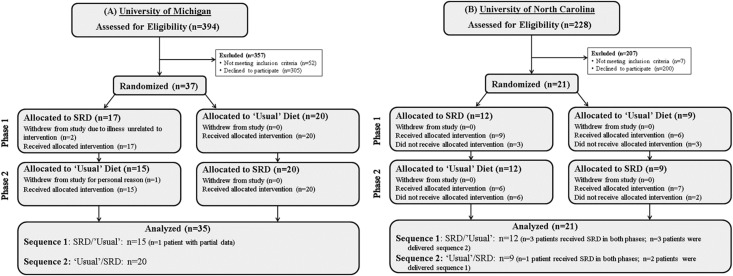
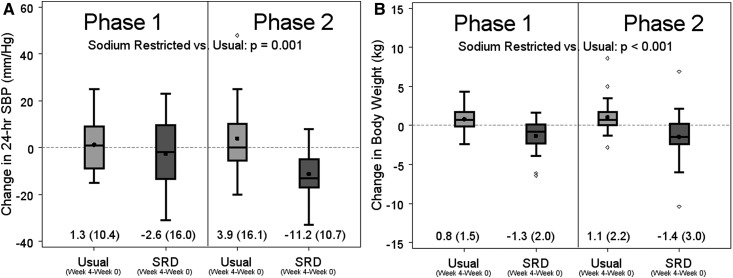
Design, setting, participants, & measurements: We conducted a randomized crossover trial to evaluate the effect of SRD (target <2 g sodium per day) versus usual diet on hydration status (by bioelectrical impedance spectroscopy) and blood pressure (BP) between May of 2009 and May of 2013. A total of 58 adults with stage 3-4 CKD were enrolled from two academic sites: University of Michigan (n=37) and University of North Carolina at Chapel Hill (n=21); 60% were men, 43% were diabetic, 93% were hypertensive, and mean age was 61 years. Participants followed SRD or usual diet for 4 weeks, followed by a 2-week washout period and a 4-week crossover phase. During the SRD, dieticians provided counseling every 2 weeks, using motivational interviewing techniques.
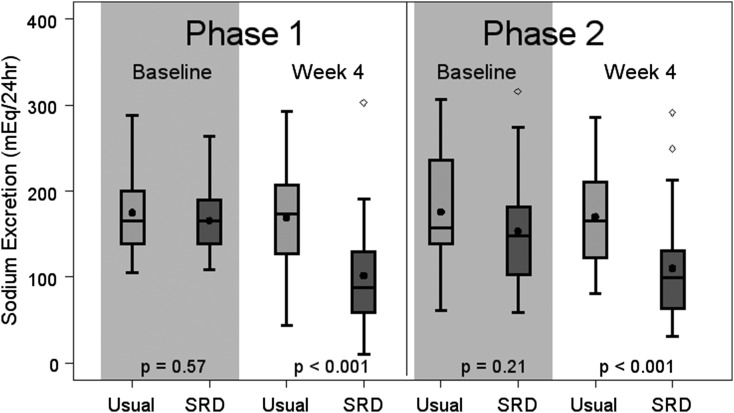
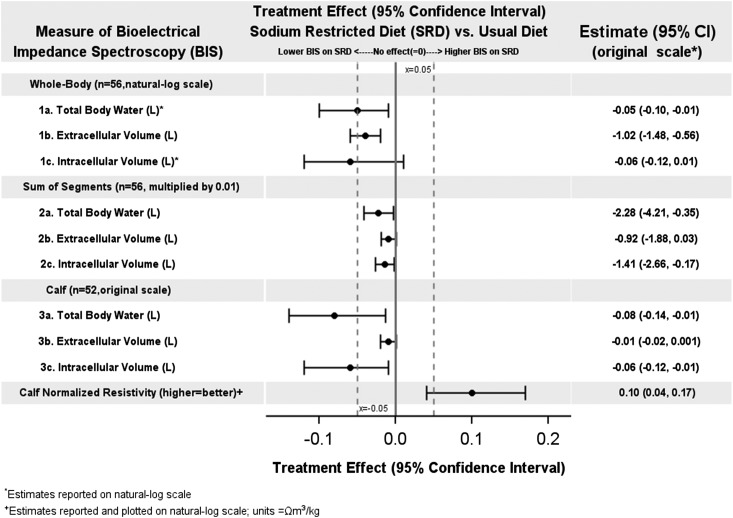
Results: Whole-body extracellular volume and calf intracellular volume decreased by 1.02 L (95% confidence interval [95% CI], -1.48 to -0.56; P<0.001) and -0.06 L (95% CI, -0.12 to -0.01; P=0.02), respectively, implying decreased fluid content on the SRD compared with usual diet. Significant reductions in urinary sodium (-57.3 mEq/24 h; 95% CI, -81.8 to -32.9), weight (-2.3 kg; 95% CI, -3.2 to -1.5), and 24-hour systolic BP (-10.8 mmHg; 95% CI, -17.0 to -4.6) were also observed (all P<0.01). Albumin-to-creatinine ratio did not change significantly and mean serum creatinine increased slightly (0.1 mg/dl; 95% CI, -0.01 to 0.2; P=0.06). No period or carryover effects were observed. Results were similar when analyzed from phase 1 only before crossover, although P values were modestly larger because of the loss of power.
Conclusions: In this randomized crossover trial, implementation of SRD in patients with CKD stage 3-4 resulted in clinically and statistically significant improvement in BP and hydration status. This simple dietary intervention merits a larger trial in CKD to evaluate effects on major clinical outcomes.
Keywords: ambulatory blood pressure monitoring; bioelectrical impedance; crossover design; motivational interviewing; salt sensitivity.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Horowitz B, Miskulin D, Zager P: Epidemiology of hypertension in CKD. Adv Chronic Kidney Dis 22: 88–95, 2015 - PubMed
-
- Heerspink HL, Ritz E: Sodium chloride intake: Is lower always better? J Am Soc Nephrol 23: 1136–1139, 2012 - PubMed
-
- Townsend RR, Taler SJ: Management of hypertension in chronic kidney disease. Nat Rev Nephrol 11: 555–563, 2015 - PubMed
-
- Sachdeva A, Weder AB: Nocturnal sodium excretion, blood pressure dipping, and sodium sensitivity. Hypertension 48: 527–533, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
