

Global impact of bronchiectasis and cystic fibrosis
- PMID: 28210295
- PMCID: PMC5298141
- DOI: 10.1183/20734735.007516
Global impact of bronchiectasis and cystic fibrosis
Abstract
Educational aims: To recognise the clinical and radiological presentation of the spectrum of diseases associated with bronchiectasis.To understand variation in the aetiology, microbiology and burden of bronchiectasis and cystic fibrosis across different global healthcare systems.
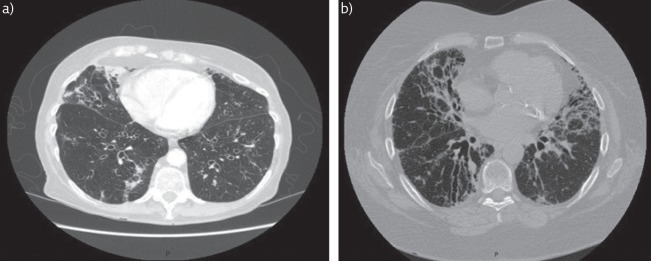
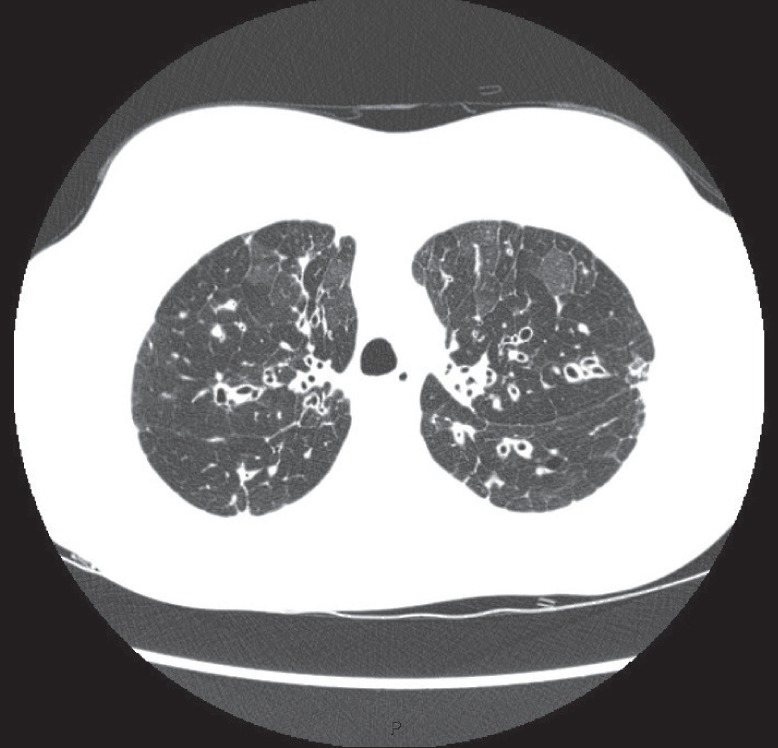
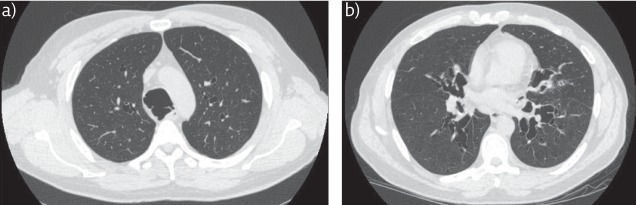
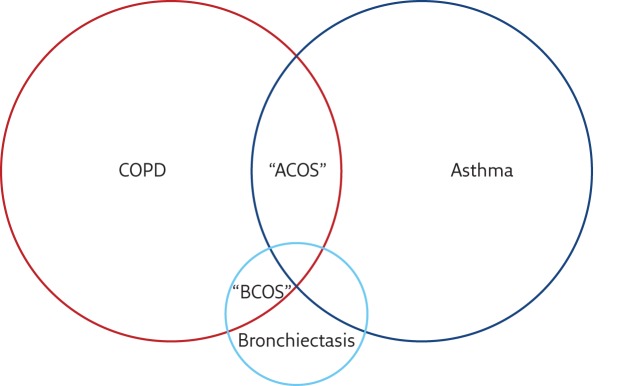
Bronchiectasis is the term used to refer to dilatation of the bronchi that is usually permanent and is associated with a clinical syndrome of cough, sputum production and recurrent respiratory infections. It can be caused by a range of inherited and acquired disorders, or may be idiopathic in nature. The most well recognised inherited disorder in Western countries is cystic fibrosis (CF), an autosomal recessive condition that leads to progressive bronchiectasis, bacterial infection and premature mortality. Both bronchiectasis due to CF and bronchiectasis due to other conditions are placing an increasing burden on healthcare systems internationally. Treatments for CF are becoming more effective leading to more adult patients with complex healthcare needs. Bronchiectasis not due to CF is becoming increasingly recognised, particularly in the elderly population. Recognition is important and can lead to identification of the underlying cause, appropriate treatment and improved quality of life. The disease is highly diverse in its presentation, requiring all respiratory physicians to have knowledge of the different "bronchiectasis syndromes". The most common aetiologies and presenting syndromes vary depending on geography, with nontuberculous mycobacterial disease predominating in some parts of North America, post-infectious and idiopathic disease predominating in Western Europe, and post-tuberculosis bronchiectasis dominating in South Asia and Eastern Europe. Ongoing global collaborative studies will greatly advance our understanding of the international impact of bronchiectasis and CF.
Conflict of interest statement
Conflict of interest Disclosures can be found alongside this article at breathe.ersjournals.com
Figures
References
-
- Pasteur MC, Bilton D, Hill AT. British Thoracic Society guideline for non-CF bronchiectasis. Thorax 2010; 65: Suppl., i1–i58. - PubMed
-
- Chalmers JD, Aliberti S, Blasi F. Treatment of bronchiectasis in adults. Eur Respir J 2015; 45: 1446–1462. - PubMed
-
- Amaral RH, Schuler Nin C, de Souza VV, et al. . Computed tomography in the diagnosis of bronchiectasis. Eur Respir J 2015; 46: 576–577. - PubMed
-
- Matsuoka S, Uchiyama K, Shima H, et al. . Bronchoarterial ratio and bronchial wall thickness on high-resolution CT in asymptomatic subjects: correlation with age and smoking. AJR Am J Roentgenol 2003; 180: 513–518. - PubMed
-
- Reiff DB, Wells AU, Carr DH, et al. . CT findings in bronchiectasis: limited value in distinguishing between idiopathic and specific types. AJR Am J Roentgenol 1995; 165: 261–267. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical