

Physiology of respiratory disturbances in muscular dystrophies
- PMID: 28210319
- PMCID: PMC5297947
- DOI: 10.1183/20734735.012716
Physiology of respiratory disturbances in muscular dystrophies
Abstract
Muscular dystrophy is a group of inherited myopathies characterised by progressive skeletal muscle wasting, including of the respiratory muscles. Respiratory failure, i.e. when the respiratory system fails in its gas exchange functions, is a common feature in muscular dystrophy, being the main cause of death, and it is a consequence of lung failure, pump failure or a combination of the two. The former is due to recurrent aspiration, the latter to progressive weakness of respiratory muscles and an increase in the load against which they must contract. In fact, both the resistive and elastic components of the work of breathing increase due to airway obstruction and chest wall and lung stiffening, respectively. The respiratory disturbances in muscular dystrophy are restrictive pulmonary function, hypoventilation, altered thoracoabdominal pattern, hypercapnia, dyspnoea, impaired regulation of breathing, inefficient cough and sleep disordered breathing. They can be present at different rates according to the type of muscular dystrophy and its progression, leading to different onset of each symptom, prognosis and degree of respiratory involvement.
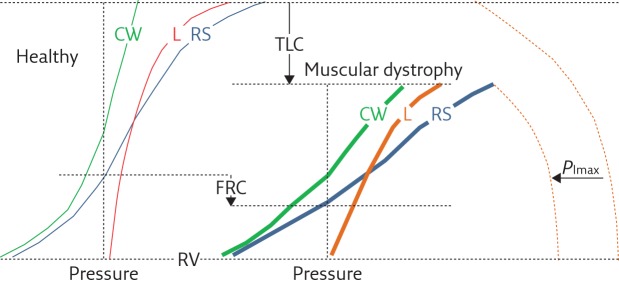
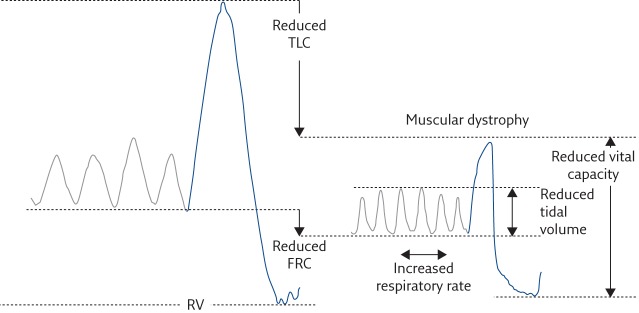
Key points: A common feature of muscular dystrophy is respiratory failure, i.e. the inability of the respiratory system to provide proper oxygenation and carbon dioxide elimination.In the lung, respiratory failure is caused by recurrent aspiration, and leads to hypoxaemia and hypercarbia.Ventilatory failure in muscular dystrophy is caused by increased respiratory load and respiratory muscles weakness.Respiratory load increases in muscular dystrophy because scoliosis makes chest wall compliance decrease, atelectasis and fibrosis make lung compliance decrease, and airway obstruction makes airway resistance increase.The consequences of respiratory pump failure are restrictive pulmonary function, hypoventilation, altered thoracoabdominal pattern, hypercapnia, dyspnoea, impaired regulation of breathing, inefficient cough and sleep disordered breathing.
Educational aims: To understand the mechanisms leading to respiratory disturbances in patients with muscular dystrophy.To understand the impact of respiratory disturbances in patients with muscular dystrophy.To provide a brief description of the main forms of muscular dystrophy with their respiratory implications.
Conflict of interest statement
Conflict of interest None declared.
Figures


References
-
- Emery AEH. The muscular dystrophies. Lancet 2002; 359: 687–695. - PubMed
-
- Perrin C, Unterborn JN, Ambrosio CD, et al. Pulmonary complications of chronic neuromuscular diseases and their management. Muscle Nerve 2004; 29: 5–27. - PubMed
-
- Allen J. Pulmonary complications of neuromuscular disease: A Respiratory mechanics perspective. Paediatr Respir Rev 2010; 11: 18–23. - PubMed
-
- De Troyer A. Respiratory effect of the lower rib displacement produced by the diaphragm. J Appl Physiol 2012; 112: 529–534. - PubMed
-
- Criner GJ, Marchetti N. Effects of neuromuscular diseases on ventilation. In: Grippi MA, Elias JA, Fishman JA, et al. eds. Fishman’s Pulmonary Diseases and Disorders. 5th Edn New York, McGraw-Hill Medical, 2015; pp. 1289–1311.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical