

Estimating the Cost of Care for Emergency Department Syncope Patients: Comparison of Three Models
- PMID: 28210361
- PMCID: PMC5305134
- DOI: 10.5811/westjem.2016.10.31171
Estimating the Cost of Care for Emergency Department Syncope Patients: Comparison of Three Models
Abstract
Introduction: We sought to compare three hospital cost-estimation models for patients undergoing evaluation for unexplained syncope using hospital cost data. Developing such a model would allow researchers to assess the value of novel clinical algorithms for syncope management.
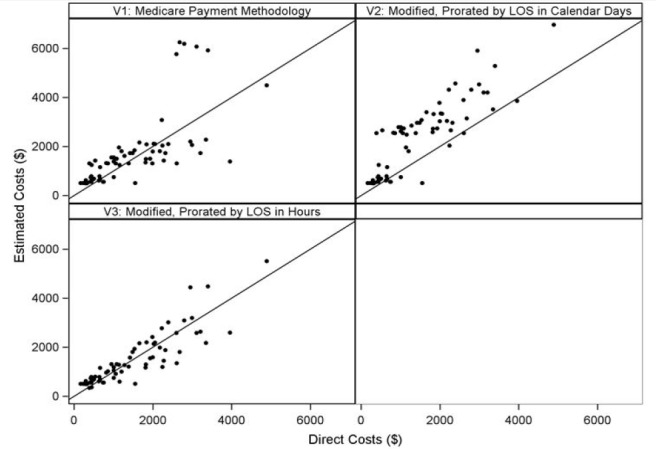
Methods: We collected complete health services data, including disposition, testing, and length of stay (LOS), on 67 adult patients (age 60 years and older) who presented to the emergency department (ED) with syncope at a single hospital. Patients were excluded if a serious medical condition was identified. We created three hospital cost-estimation models to estimate facility costs: V1, unadjusted Medicare payments for observation and/or hospital admission; V2: modified Medicare payment, prorated by LOS in calendar days; and V3: modified Medicare payment, prorated by LOS in hours. Total hospital costs included unadjusted Medicare payments for diagnostic testing and estimated facility costs. We plotted these estimates against actual cost data from the hospital finance department, and performed correlation and regression analyses.
Results: Of the three models, V3 consistently outperformed the others with regard to correlation and goodness of fit. The Pearson correlation coefficient for V3 was 0.88 (95% confidence interval [CI] 0.81, 0.92) with an R-square value of 0.77 and a linear regression coefficient of 0.87 (95% CI 0.76, 0.99).
Conclusion: Using basic health services data, it is possible to accurately estimate hospital costs for older adults undergoing a hospital-based evaluation for unexplained syncope. This methodology could help assess the potential economic impact of implementing novel clinical algorithms for ED syncope.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. This project was supported by a grant from the NIH/NHLBI: R01 HL111033. Marc A. Probst is supported by a grant from the NIH/NHLBI: 1K23HL132052-01. Michelle P. Lin is supported by a grant from the Emergency Medicine Foundation.
Figures
References
-
- Porter ME. What is value in health care? N Engl J Med. 2010;363:2477–81. - PubMed
-
- National Priorities Partnership. Reducing Emergency Department Overuse: A $38 Billion Opportunity. Massachusetts: 2011. [Accessed Jan 24, 2016]. National Quality Forum. Available at: www.nehi.net/bendthecurve/sup/documents/ED_Overuse_Brief.pdf. 2015.
-
- Sun BC, Emond JA, Camargo CA., Jr Direct medical costs of syncope-related hospitalizations in the United States. Am J Cardiol. 2005;95:668–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases