

Case Reports
doi: 10.1055/s-0036-1584402.
Epub 2016 Jun 22.
Reconstruction of a Combined Maxillectomy and Segmental Mandibulectomy Defect in a Seven-Year-Old with a Single Free Fibula Osteocutaneous Flap
Affiliations
- PMID: 28210412
- PMCID: PMC5305311
- DOI: 10.1055/s-0036-1584402
Item in Clipboard
Case Reports
Reconstruction of a Combined Maxillectomy and Segmental Mandibulectomy Defect in a Seven-Year-Old with a Single Free Fibula Osteocutaneous Flap
Craniomaxillofac Trauma Reconstr.
2017 Mar.
Abstract
Combined upper alveolectomy and segmental mandibulectomy are complex defects. Reconstruction of these defects is usually suboptimal. We describe the case of a pediatric patient with vessel-depleted neck with recurrent vascular malformation involving the ramus and coronoid process of mandible and a previous history of maxillectomy and a reconstruction with anterolateral thigh flap. The patient underwent wide resection. The defects involving the upper alveolus and mandible were simultaneously reconstructed with a single free fibula flap.
Keywords: combined maxilla and mandible defect; fibula flap; mandibular reconstruction; maxillary reconstruction; pediatric patient.
Figures

Preoperative frontal view photograph of the patient, prior to the latest surgery.
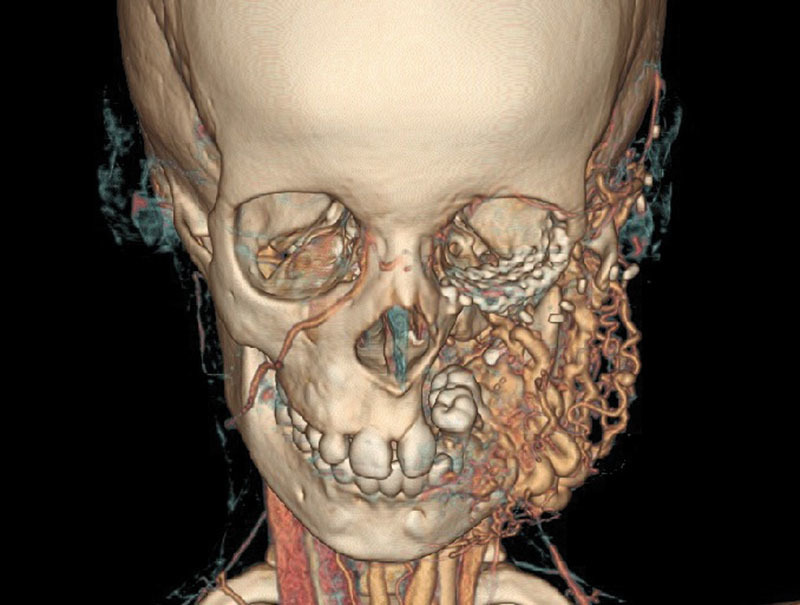
Three dimensional CT scan with angiogram showing the lesion involving the ramus and coronoid region of left hemi-mandible with feeders from left external carotid artery.

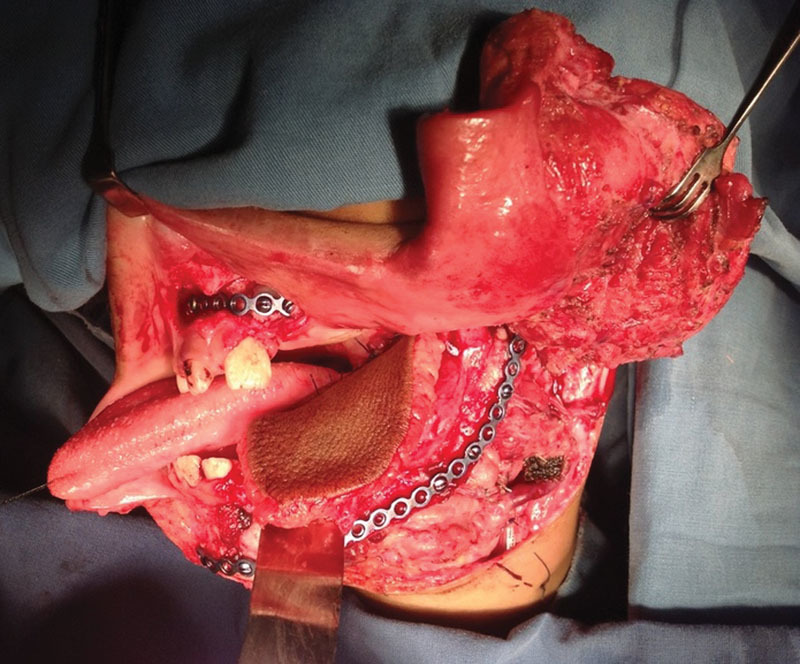
Postresection photograph showing segmental mandibulectomy defect, with preservation of a part of vertical ramus and condyle to which the plate has been attached. Note the upper alveolus defect, which has been reconstructed only with a soft-tissue flap.

Fibula flap with the design for reconstruction. The intervening bone segment has been removed keeping the periosteum in continuity.
Flap inset has been done to reconstruct the defect. The upper segment of the fibula has been fixed to the upper alveolus stump and the lower segments used to reconstruct the mandible.
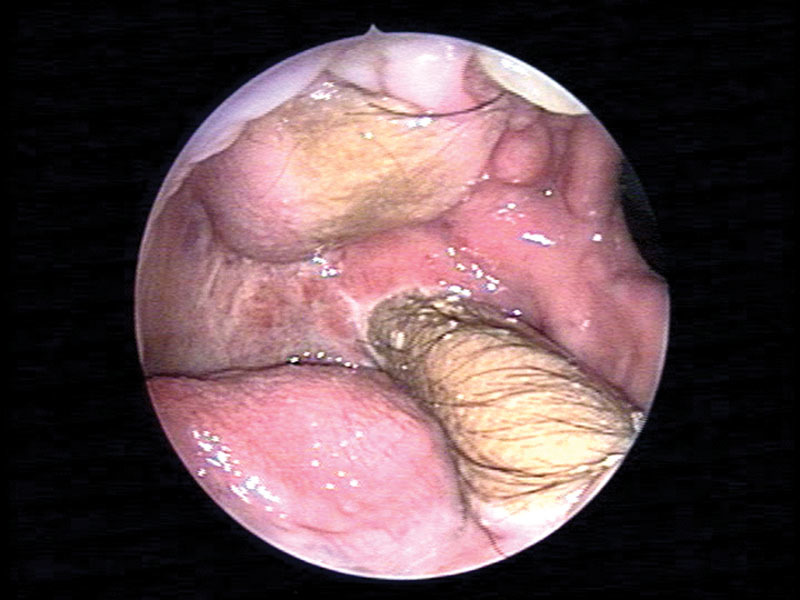
Endoscopic view of oral cavity showing the status 6 months postoperatively.

Frontal view of the patient 24 months after surgery.
Similar articles
-
Oral rehabilitation for patients with marginal and segmental mandibulectomy: A retrospective review of 111 mandibular resection prostheses.J Prosthet Dent. 2019 Jul;122(1):82-87. doi: 10.1016/j.prosdent.2018.09.020. Epub 2019 Feb 16. J Prosthet Dent. 2019. PMID: 30782457 Free PMC article.
-
Ramus to Ramus Mandibular Defect Reconstruction with Osteocutaneous Fibula Free Flap - Case Presentation.Maedica (Bucur). 2020 Sep;15(3):401-408. doi: 10.26574/maedica.2020.15.3.401. Maedica (Bucur). 2020. PMID: 33312259 Free PMC article.
-
A 20-year experience of immediate mandibular reconstruction using free fibula osteocutaneous flaps following ameloblastoma resection: Radical resection, outcomes, and recurrence.Arch Plast Surg. 2019 Sep;46(5):426-432. doi: 10.5999/aps.2018.01487. Epub 2019 Sep 15. Arch Plast Surg. 2019. PMID: 31550747 Free PMC article.
-
A systematic review of validated tools assessing functional and aesthetic outcomes following fibula free flap reconstruction of the mandible.Head Neck. 2019 Jan;41(1):248-255. doi: 10.1002/hed.25452. Epub 2018 Dec 12. Head Neck. 2019. PMID: 30548509 Free PMC article.
-
Reconstruction options in pediatric population with hemi or total mandibulectomy defects: A systematic review.J Oral Biol Craniofac Res. 2022 Mar-Apr;12(2):238-247. doi: 10.1016/j.jobcr.2022.03.001. Epub 2022 Mar 16. J Oral Biol Craniofac Res. 2022. PMID: 35313656 Free PMC article. Review.
Cited by
-
Fibula Musculo-Osteocutaneous Flap with Full Thickness of Flexor Hallucis Longus Muscle.World J Plast Surg. 2021 Jan;10(1):22-29. doi: 10.29252/wjps.10.1.22. World J Plast Surg. 2021. PMID: 33833950 Free PMC article.
References
-
- Thankappan K, Trivedi N P, Subash P. et al.Three-dimensional computed tomography-based contouring of a free fibula bone graft for mandibular reconstruction. J Oral Maxillofac Surg. 2008;66(10):2185–2192. - PubMed
-
- Punpale A S, Rajendra Prasad J S, Shetty K P, Kadam S, Udupa V. An innovative design for simultaneous reconstruction of complex maxillo-mandibular defects with single free fibula osteocutaneous flap. J Plast Reconstr Aesthet Surg. 2006;59(1):96–101. - PubMed
-
- Laure B, Sury F, Martin T, Chabut A, Goga D. Reconstruction of bony mandibular and maxillary defects with one single transfer of a free fibula osteocutaneous flap. J Plast Reconstr Aesthet Surg. 2008;61(2):200–203. - PubMed
-
- Sadove R C, Powell L A. Simultaneous maxillary and mandibular reconstruction with one free osteocutaneous flap. Plast Reconstr Surg. 1993;92(1):141–146. - PubMed
-
- Ozkan O, Ozgentas H E, Dikici M B. Simultaneous reconstruction of large maxillary and mandibular defects with a fibular osteocutaneous flap combined with an anterolateral thigh flap. J Reconstr Microsurg. 2004;20(6):451–455. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources