

Postoperative Rehabilitation After Rotator Cuff Repair: A Web-Based Survey of AANA and AOSSM Members
- PMID: 28210654
- PMCID: PMC5302103
- DOI: 10.1177/2325967116684775
Postoperative Rehabilitation After Rotator Cuff Repair: A Web-Based Survey of AANA and AOSSM Members
Abstract
Background: Postoperative rehabilitation after arthroscopic rotator cuff repair (ARCR) remains controversial and suffers from limited high-quality evidence. Therefore, appropriate use criteria must partially depend on expert opinion.
Hypothesis/purpose: The purpose of the study was to determine and report on the standard and modified rehabilitation protocols after ARCR used by member orthopaedic surgeons of the American Orthopaedic Society for Sports Medicine (AOSSM) and the Arthroscopy Association of North America (AANA). We hypothesized that there will exist a high degree of variability among rehabilitation protocols. We also predict that surgeons will be prescribing accelerated rehabilitation.
Study design: Cross-sectional study; Level of evidence, 4.
Methods: A 29-question survey in English language was sent to all 3106 associate and active members of the AOSSM and the AANA. The questionnaire consisted of 4 categories: standard postoperative protocol, modification to postoperative rehabilitation, operative technique, and surgeon demographic data. Via email, the survey was sent on September 4, 2013.
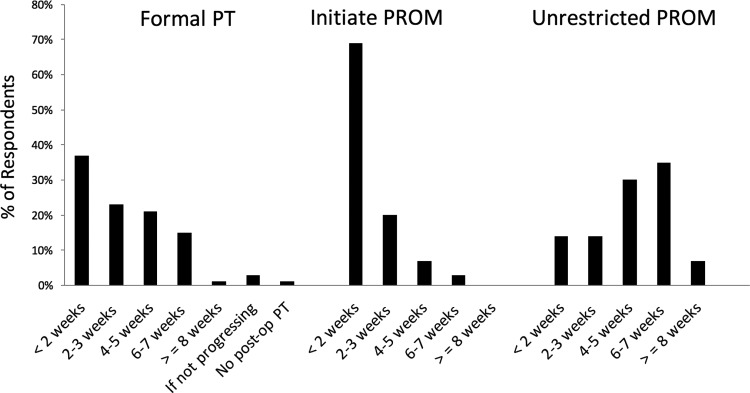
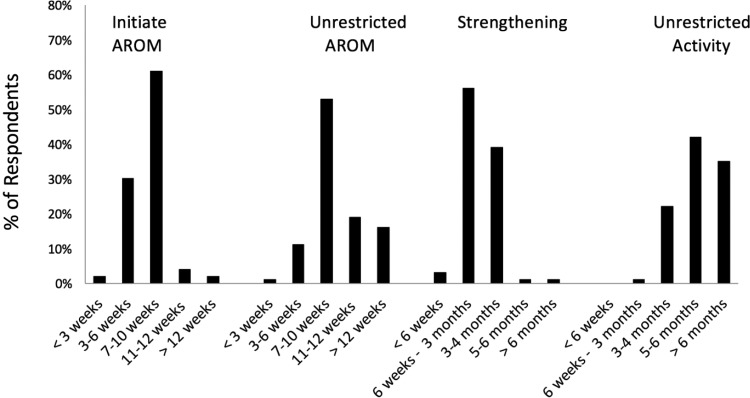
Results: The average response rate per question was 22.7%, representing an average of 704 total responses per question. The most common immobilization device was an abduction pillow sling with the arm in neutral or slight internal rotation (70%). Surgeons tended toward later unrestricted passive shoulder range of motion at 6 to 7 weeks (35%). Strengthening exercises were most commonly prescribed between 6 weeks and 3 months (56%). Unrestricted return to activities was most commonly allowed at 5 to 6 months. The majority of the respondents agreed that they would change their protocol based on differences expressed in this survey.
Conclusion: There is tremendous variability in postoperative rehabilitation protocols after ARCR. Five of 10 questions regarding standard rehabilitation reached a consensus statement. Contrary to our hypothesis, there was a trend toward later mobilization.
Keywords: ARCR; arthroscopic; general; physical therapy/rehabilitation; rotator cuff; shoulder.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Figures
References
-
- Bishop YJ, Santiago-Torres JE, Rimmke N, Flanigan DC. Smoking predisposes to rotator cuff pathology and shoulder dysfunction: a systematic review. Arthroscopy. 2015;31:1598–1605. - PubMed
-
- Cuff DJ, Pupello DR. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. J Shoulder Elbow Surg. 2012;21:1450–1455. - PubMed
-
- Denard PJ, Jiwani AZ, Ladermann A, Burkhart SS. Long-term outcome of arthroscopic massive rotator cuff repair: the importance of double-row fixation. Arthroscopy. 2012;28:909–915. - PubMed
-
- Keener JD, Galatz LM, Stobbs-Cucchi G, Patton R, Yamaguchi K. Rehabilitation following arthroscopic rotator cuff repair: a prospective randomized trial of immobilization compared with early motion. J Bone Joint Surg Am. 2014;96:11–19. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
