

Decoding the Molecular and Mutational Ambiguities of Gastroenteropancreatic Neuroendocrine Neoplasm Pathobiology
- PMID: 28210673
- PMCID: PMC5301133
- DOI: 10.1016/j.jcmgh.2014.12.008
Decoding the Molecular and Mutational Ambiguities of Gastroenteropancreatic Neuroendocrine Neoplasm Pathobiology
Abstract
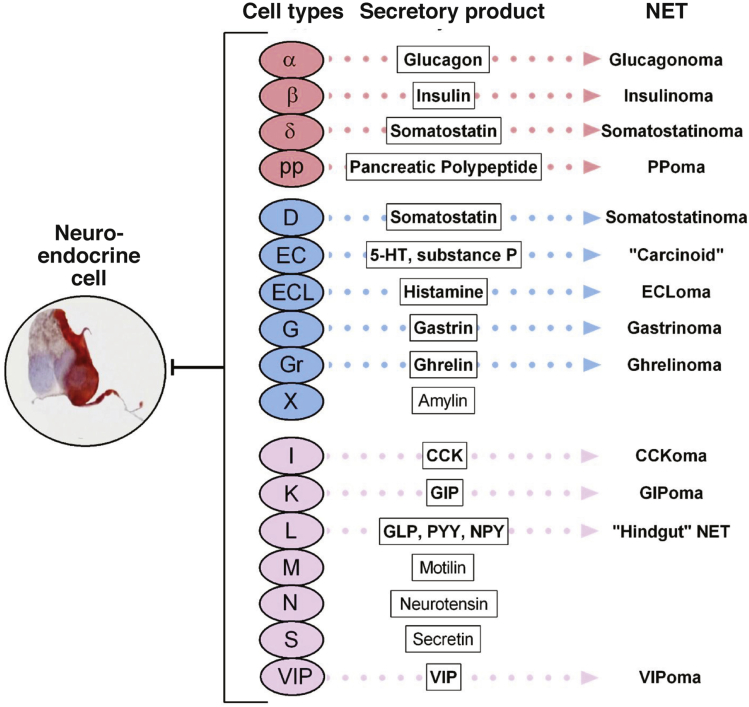
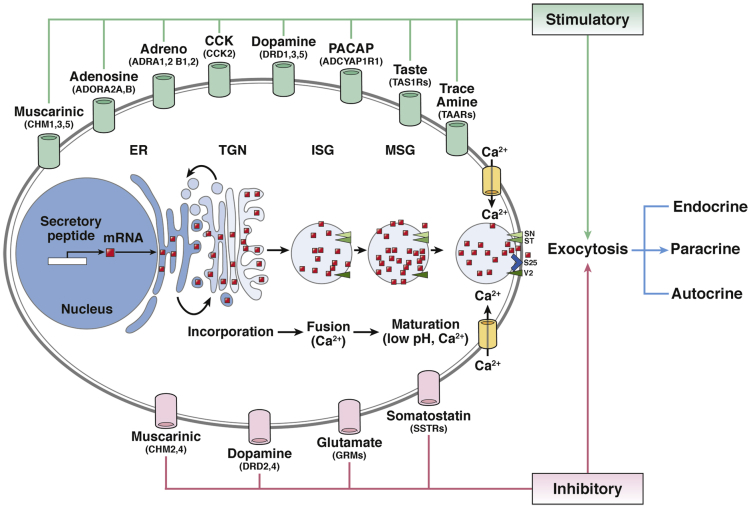
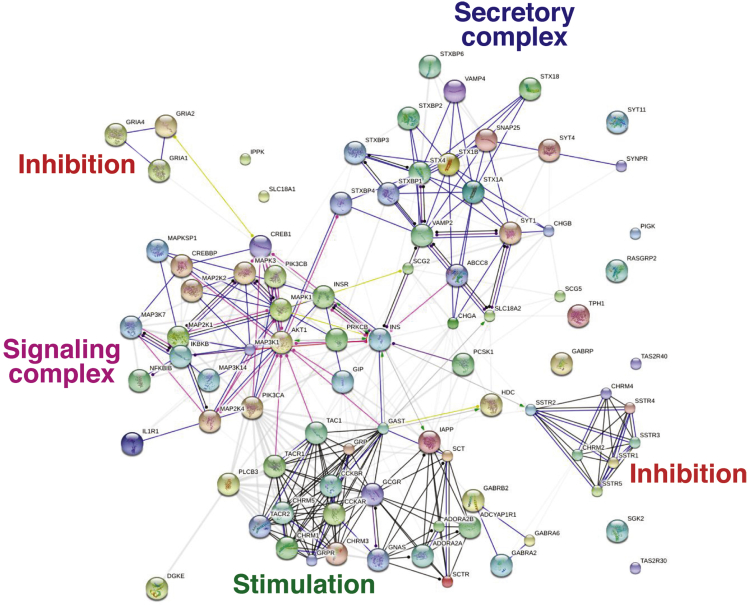
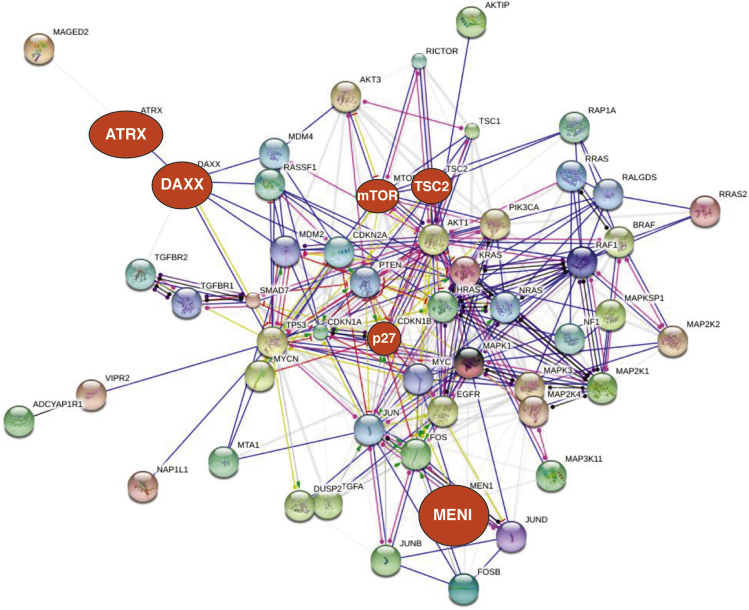
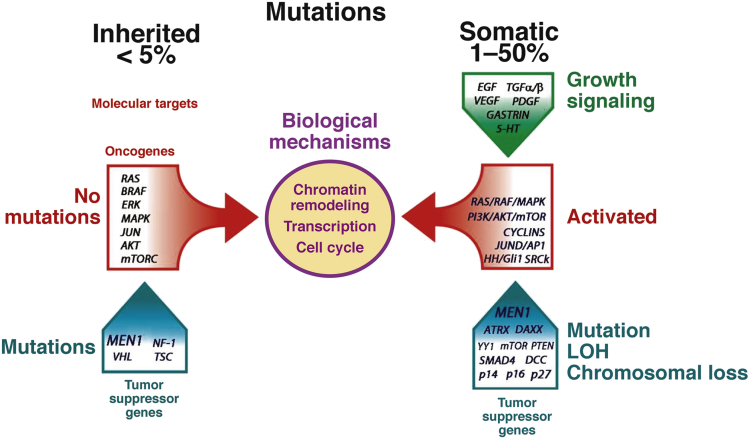
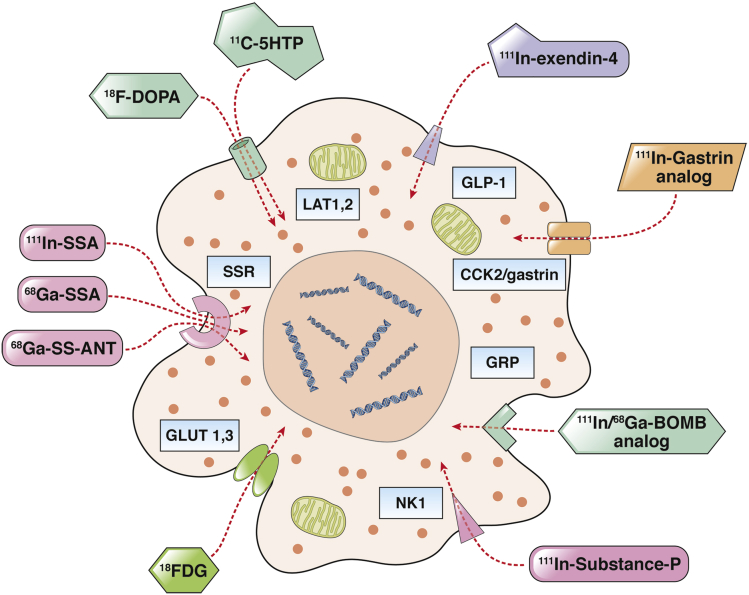
Gastroenteropancreatic neuroendocrine neoplasms (GEP-NEN), considered a heterogeneous neoplasia, exhibit ill-defined pathobiology and protean symptomatology and are ubiquitous in location. They are difficult to diagnose, challenging to manage, and outcome depends on cell type, secretory product, histopathologic grading, and organ of origin. A morphologic and molecular genomic review of these lesions highlights tumor characteristics that can be used clinically, such as somatostatin-receptor expression, and confirms features that set them outside the standard neoplasia paradigm. Their unique pathobiology is useful for developing diagnostics using somatostatin-receptor targeted imaging or uptake of radiolabeled amino acids specific to secretory products or metabolism. Therapy has evolved via targeting of protein kinase B signaling or somatostatin receptors with drugs or isotopes (peptide-receptor radiotherapy). With DNA sequencing, rarely identified activating mutations confirm that tumor suppressor genes are relevant. Genomic approaches focusing on cancer-associated genes and signaling pathways likely will remain uninformative. Their uniquely dissimilar molecular profiles mean individual tumors are unlikely to be easily or uniformly targeted by therapeutics currently linked to standard cancer genetic paradigms. The prevalence of menin mutations in pancreatic NEN and P27KIP1 mutations in small intestinal NEN represents initial steps to identifying a regulatory commonality in GEP-NEN. Transcriptional profiling and network-based analyses may define the cellular toolkit. Multianalyte diagnostic tools facilitate more accurate molecular pathologic delineations of NEN for assessing prognosis and identifying strategies for individualized patient treatment. GEP-NEN remain unique, poorly understood entities, and insight into their pathobiology and molecular mechanisms of growth and metastasis will help identify the diagnostic and therapeutic weaknesses of this neoplasia.
Keywords: 5-HT, serotonin, 5-hydroxytryptamine; Akt, protein kinase B; BRAF, gene encoding serine/threonine-protein kinase B-Raf; Blood; CGH, comparative genomic hybridization; CREB, cAMP response element-binding protein; Carcinoid; CgA, chromogranin A; D cell, somatostatin; DAG, diacylglycerol; EC, enterochromaffin; ECL, enterochromaffin-like; EGFR, epidermal growth factor receptor; ERK, extracellular-signal-regulated kinase; G cell, gastrin; GABA, γ-aminobutyric acid; GEP-NEN, gastroenteropancreatic neuroendocrine neoplasms; GPCR, G-protein coupled receptor; Gastroenteropancreatic Neuroendocrine Neoplasms; IGF-I, insulin-like growth factor-I; ISG, immature secretory vesicles; Ki-67; LOH, loss of heterozygosity; MAPK, mitogen-activated protein kinase; MEN-1/MEN1, multiple endocrine neoplasia type 1; MSI, microsatellite instability; MTA, metastasis associated-1; NEN, neuroendocrine neoplasms; NFκB, nuclear factor κB; PET, positron emission tomography; PI3, phosphoinositide-3; PI3K, phosphoinositide-3 kinase; PKA, protein kinase A; PKC, protein kinase C; PTEN, phosphatase and tensin homolog deleted on chromosome 10; Proliferation; SD-208, 2-(5-chloro-2-fluorophenyl)-4-[(4-pyridyl)amino]p-teridine; SNV, single-nucleotide variant; SSA, somatostatin analog; SST, somatostatin; Somatostatin; TGF, transforming growth factor; TGN, trans-Golgi network; TSC2, tuberous sclerosis complex 2 (tuberin); Transcriptome; VMAT, vesicular monoamine transporters; X/A-like cells, ghrelin; cAMP, adenosine 3′,5′-cyclic monophosphate; mTOR, mammalian target of rapamycin; miR/miRNA, micro-RNA.
Figures
References
-
- Modlin I.M., Oberg K., Chung D.C. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008;9:61–72. - PubMed
-
- Strosberg J. Evolving treatment strategies for management of carcinoid tumors. Curr Treat Options Oncol. 2013;14:374–388. - PubMed
-
- Baudin E., Planchard D., Scoazec J.Y. Intervention in gastro-enteropancreatic neuroendocrine tumours. Best Pract Res Clin Gastroenterol. 2012;26:855–865. - PubMed
-
- Modlin I.M., Kidd M., Latich I. Current status of gastrointestinal carcinoids. Gastroenterology. 2005;128:1717–1751. - PubMed
-
- Yao J.C., Hassan M., Phan A. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008;26:3063–3072. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
