

Deep Phenotyping of Systemic Arterial Hemodynamics in HFpEF (Part 1): Physiologic and Technical Considerations
- PMID: 28210939
- PMCID: PMC5515681
- DOI: 10.1007/s12265-017-9735-3
Deep Phenotyping of Systemic Arterial Hemodynamics in HFpEF (Part 1): Physiologic and Technical Considerations
Erratum in
-
Erratum to: Deep Phenotyping of Systemic Arterial Hemodynamics in HFpEF (Part 1): Physiologic and Technical Considerations.J Cardiovasc Transl Res. 2017 Jun;10(3):260. doi: 10.1007/s12265-017-9745-1. J Cardiovasc Transl Res. 2017. PMID: 28432533 No abstract available.
Abstract
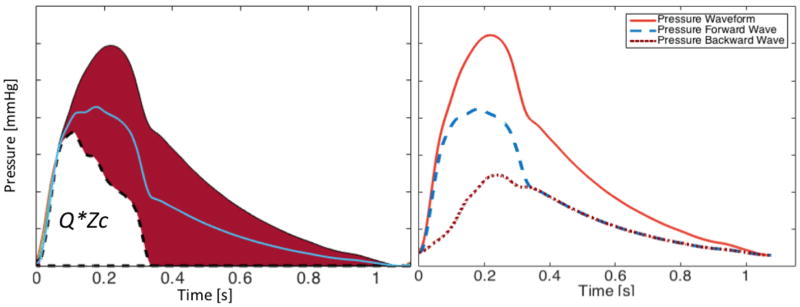
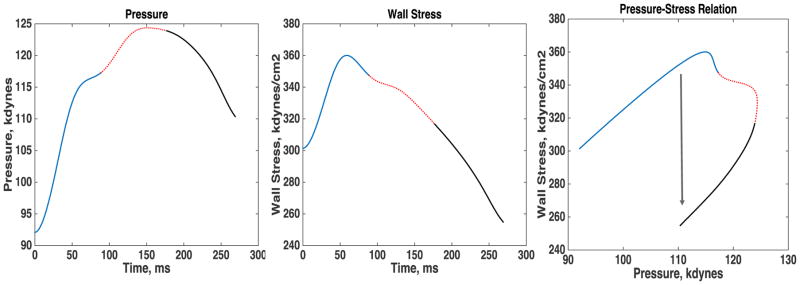
A better understanding of the pathophysiology of heart failure with a preserved left ventricular ejection fraction (HFpEF) is important. Detailed phenotyping of pulsatile hemodynamics has provided important insights into the pathophysiology of left ventricular remodeling and fibrosis, diastolic dysfunction, microvascular disease, and impaired oxygen delivery to peripheral skeletal muscle, all of which contribute to exercise intolerance, the cardinal feature of HFpEF. Furthermore, arterial pulsatile hemodynamic mechanisms likely contribute to the frequent presence of comorbidities, such as renal failure and dementia, in this population. Our therapeutic approach to HFpEF can be enhanced by clinical phenotyping tools with the potential to "segment" this population into relevant pathophysiologic categories or to identify individuals exhibiting prominent specific abnormalities that can be targeted by pharmacologic interventions. This review describes relevant technical and physiologic aspects regarding the deep phenotyping of arterial hemodynamics in HFpEF. In an accompanying review, the potential of this approach to enhance our clinical and therapeutic approach to HFpEF is discussed.
Keywords: Afterload; Arterial hemodynamics; Heart failure; Heart failure with preserved ejection fraction; Pulsatile load; Wave reflections.
Figures

References
-
- Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, Greenlund K, Daniels S, Nichol G, Tomaselli GF, Arnett DK, Fonarow GC, Ho PM, Lauer MS, Masoudi FA, Robertson RM, Roger V, Schwamm LH, Sorlie P, Yancy CW, Rosamond WD. Defining and setting national goals for cardiovascular health promotion and disease reduction: The american heart association's strategic impact goal through 2020 and beyond. Circulation. 2010;121:586–613. - PubMed
-
- Cleland JG, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J. The perindopril in elderly people with chronic heart failure (pep-chf) study. Eur Heart J. 2006;27:2338–2345. - PubMed
-
- Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, Anderson S, Donovan M, Iverson E, Staiger C, Ptaszynska A. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359:2456–2467. - PubMed
-
- Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, Michelson EL, Olofsson B, Ostergren J. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: The charm-preserved trial. Lancet. 2003;362:777–781. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
