

Joint reconstruction of Ictal/inter-ictal SPECT data for improved epileptic foci localization
- PMID: 28211105
- PMCID: PMC5462456
- DOI: 10.1002/mp.12167
Joint reconstruction of Ictal/inter-ictal SPECT data for improved epileptic foci localization
Abstract
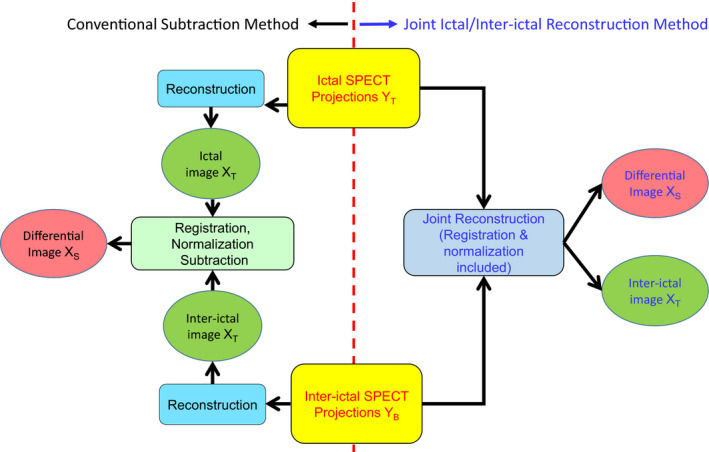
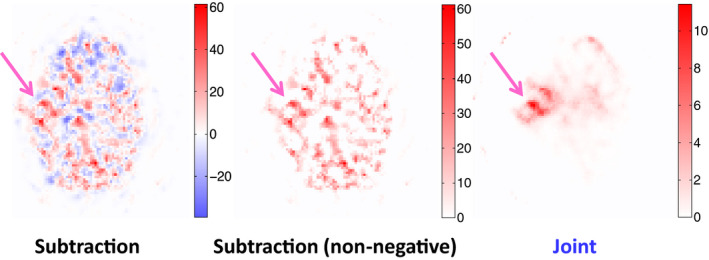
Purpose: To improve the performance for localizing epileptic foci, we have developed a joint ictal/inter-ictal SPECT reconstruction method in which ictal and inter-ictal SPECT projections are simultaneously reconstructed to obtain the differential image.
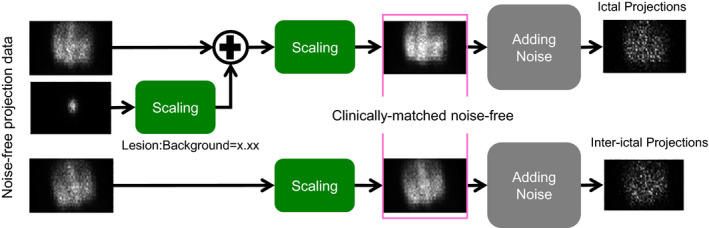
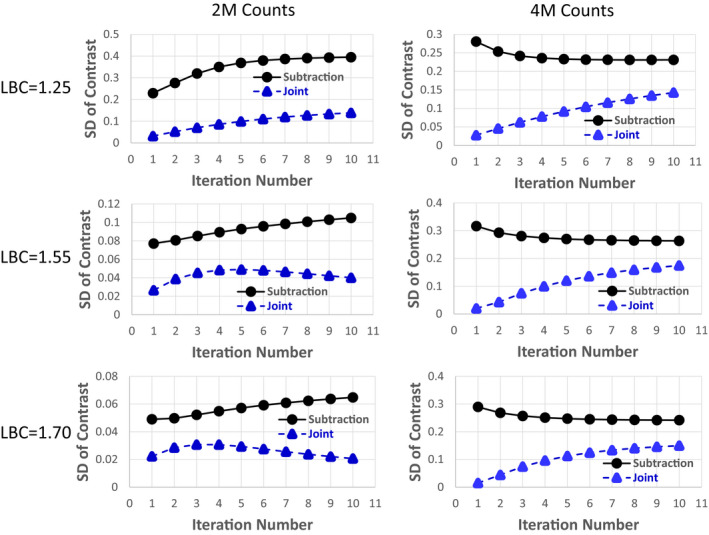
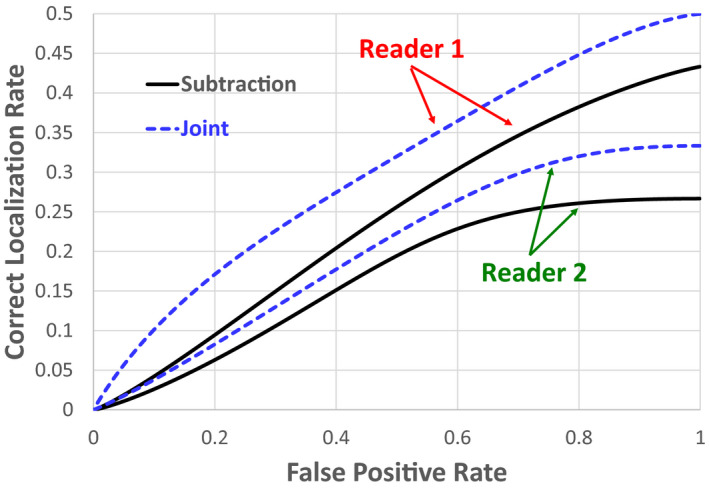
Methods: We have developed a SPECT reconstruction method that jointly reconstructs ictal and inter-ictal SPECT projection data. We performed both phantom and patient studies to evaluate the performance of our joint method for epileptic foci localization as compared with the conventional subtraction method in which the differential image is obtained by subtracting the inter-ictal image from the co-registered ictal image. Two low-noise SPECT projection datasets were acquired using 99m Tc and a Hoffman head phantom at two different positions and orientations. At one of the two phantom locations, a low-noise dataset was also acquired using a 99m Tc-filled 3.3-cm sphere with a cold attenuation background identical to the Hoffman phantom. These three datasets were combined and scaled to mimic low-noise clinical ictal (three different lesion-to-background contrast levels: 1.25, 1.55, and 1.70) and inter-ictal scans. For each low-noise dataset, 25 noise realizations were generated by adding Poisson noise to the projections. The mean and standard deviation (SD) of lesion contrast in the differential images were computed using both the conventional subtraction and our joint methods. We also applied both methods to the 35 epileptic patient datasets. Each differential image was presented to two nuclear medicine physicians to localize a lesion and specify a confidence level. The readers' data were analyzed to obtain the localized-response receiver operating characteristic (LROC) curves for both the subtraction and joint methods.
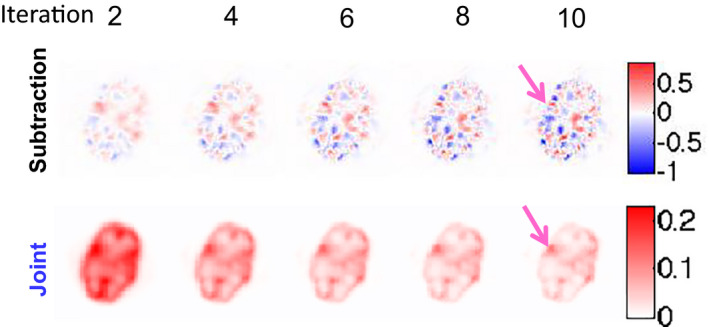
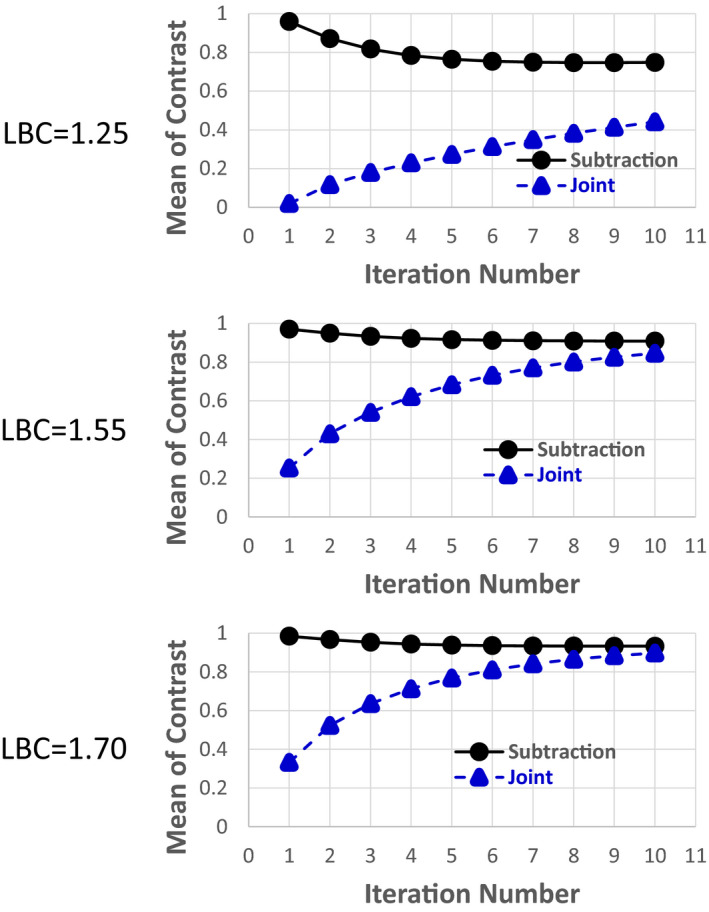
Results: For the phantom study, the difference between the mean lesion contrast in the differential images obtained using the conventional subtraction versus our joint method decreases as the iteration number increases. Compared with the conventional subtraction approach, the SD reduction of lesion contrast at the 10th iteration using our joint method ranges from 54.7% to 68.2% (P < 0.0005), and 33.8% to 47.9% (P < 0.05) for 2 and 4 million total inter-ictal counts, respectively. In the patient study, our joint method increases the area under LROC from 0.24 to 0.34 and from 0.15 to 0.20 for the first and second reader, respectively. We have demonstrated improved performance of our method as compared to the standard subtraction method currently used in clinical practice.
Conclusion: The proposed joint ictal/inter-ictal reconstruction method yields better performance for epileptic foci localization than the conventional subtraction method.
Keywords: epileptic foci localization; joint ictal/inter-ictal SPECT reconstruction.
© 2017 American Association of Physicists in Medicine.
Conflict of interest statement
The authors report no conflicts of interest in conducting this research.
Figures
Similar articles
-
Impact of reconstruction parameters on lesion detection and localization in joint ictal/inter-ictal SPECT reconstruction.Ann Nucl Med. 2022 Jan;36(1):24-32. doi: 10.1007/s12149-021-01680-x. Epub 2021 Sep 24. Ann Nucl Med. 2022. PMID: 34559366
-
Simultaneous 99mTc-MDP/123I-MIBG tumor imaging using SPECT-CT: phantom and constructed patient studies.Med Phys. 2013 Oct;40(10):102506. doi: 10.1118/1.4820977. Med Phys. 2013. PMID: 24089927 Free PMC article.
-
Use of subtraction ictal SPECT co-registered to MRI for optimizing the localization of seizure foci in children.J Nucl Med. 1999 May;40(5):786-92. J Nucl Med. 1999. PMID: 10319751
-
Preoperative parathyroid localization using joint planar imaging.Annu Int Conf IEEE Eng Med Biol Soc. 2017 Jul;2017:624-627. doi: 10.1109/EMBC.2017.8036902. Annu Int Conf IEEE Eng Med Biol Soc. 2017. PMID: 29059950
-
Subtraction ictal SPECT coregistered to MRI for seizure focus localization in partial epilepsy.Mayo Clin Proc. 2000 Jun;75(6):615-24. doi: 10.4065/75.6.615. Mayo Clin Proc. 2000. PMID: 10852423 Review.
Cited by
-
Absolute Quantification in Diagnostic SPECT/CT: The Phantom Premise.Diagnostics (Basel). 2021 Dec 11;11(12):2333. doi: 10.3390/diagnostics11122333. Diagnostics (Basel). 2021. PMID: 34943570 Free PMC article. Review.
-
Dual-Tracer Parathyroid Imaging Using Joint SPECT Reconstruction.Nucl Med Mol Imaging. 2023 Jun;57(3):126-136. doi: 10.1007/s13139-022-00787-x. Epub 2023 Jan 16. Nucl Med Mol Imaging. 2023. PMID: 37187950 Free PMC article.
-
Design and development of the DE-SPECT system: a clinical SPECT system for broadband multi-isotope imaging of peripheral vascular disease.Phys Med Biol. 2024 Jun 11;69(12):125016. doi: 10.1088/1361-6560/ad5266. Phys Med Biol. 2024. PMID: 38815617 Free PMC article.
-
Subtraction of single-photon emission computed tomography (SPECT) in radioembolization: a comparison of four methods.EJNMMI Phys. 2024 Aug 15;11(1):72. doi: 10.1186/s40658-024-00675-7. EJNMMI Phys. 2024. PMID: 39143361 Free PMC article.
-
Nuclear imaging for localization and surgical outcome prediction in epilepsy: A review of latest discoveries and future perspectives.Front Neurol. 2022 Dec 16;13:1083775. doi: 10.3389/fneur.2022.1083775. eCollection 2022. Front Neurol. 2022. PMID: 36588897 Free PMC article.
References
-
- Begley C, Beghi E, Beran R, et al. ILAE commission on the burden of epilepsy, subcommission on the economic burden of epilepsy: Final report 1998–2001. Epilepsia. 2002;43:668–673. - PubMed
-
- Yoon D, Frick K, Carr D, Austin J. Economic impact of epilepsy in the United States. Epilepsia. 2009;50:2186–2191. - PubMed
-
- Cascino G. Surgical treatment for epilepsy. Epilepsy Res. 2004;60:179–186. - PubMed
-
- Uber‐Zak L, Blum D. Epilepsy surgery: Chance for a cure. Curr Neurol Neurosci Rep. 2001;1:376–380. - PubMed
-
- Luders H, Comair Y. Epilepsy Surgery. Philadelphia: Lippincott Williams and Wikins; 2001.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
