

Primary Human Cytomegalovirus (HCMV) Infection in Pregnancy
- PMID: 28211317
- PMCID: PMC5319378
- DOI: 10.3238/arztebl.2017.0045
Primary Human Cytomegalovirus (HCMV) Infection in Pregnancy
Abstract
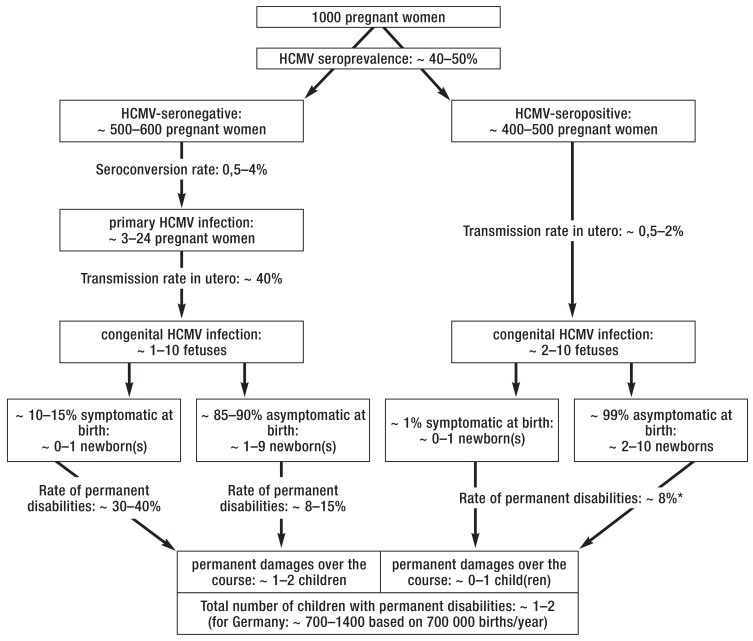
Background: In 0.5-4% of pregnancies, the prospective mother sustains a primary infection with human cytomegalovirus (HCMV). An HCMV infection of the fetus in the first or second trimester can cause complex post-encephalitic impairment of the infant brain, leading to motor and mental retardation, cerebral palsy, epilepsy, retinal defects, and progressive hearing loss.
Methods: This review is based on pertinent publications from January 2000 to October 2016 that were retrieved by a selective search in PubMed employing the terms "cytomegalovirus and pregnancy" and "congenital cytomegalovirus."
Results: 85-90% of all neonates with HCMV infection are asymptomatic at birth. The main long-term sequela is hearing impairment, which develops in 8-15% of these affected children. Hygienic measures can lower the risk of primary HCMV infection in pregnancy by 50-85%. The first randomized and controlled trial (RCT) of passive immunization with an HCMV-specific hyper - immune globulin (HIG) preparation revealed a trend toward a lower risk of congenital transmission of the virus (30% versus 44% with placebo, p = 0.13). The effect of HIG was more marked in the initial non-randomized trial (15% versus 40%, p = 0.02). The RCT also showed HIG to be associated with a higher frequency of fetal growth retardation and premature birth (13% versus 2%, p = 0.06). Valaciclovir is a further, non-approved treatment option.
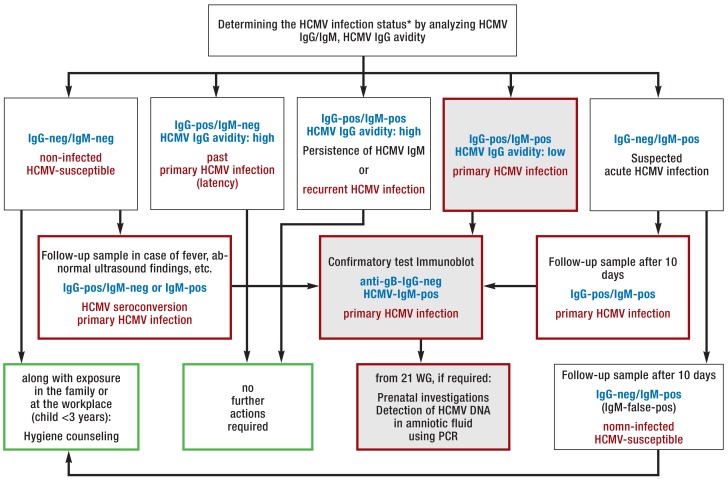
Conclusion: In the absence of an active vaccine against HCMV, counseling about hygienic measures may currently be the single most effective way to prevent congenital HCMV infection. Moreover, HCMV serologic testing is recommended in the guideline of the Association of the Scientific Medical Societies in Germany (Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften, AWMF). Further randomized trials of treatment with HIG and with valaciclovir are urgently needed so that the options for the prevention and treatment of congenital HCMV infection can be assessed.
Figures



Comment in
-
Protecting the Health of Pregnant Women.Dtsch Arztebl Int. 2017 Jul 24;114(29-30):504. doi: 10.3238/arztebl.2017.0504a. Dtsch Arztebl Int. 2017. PMID: 28818180 Free PMC article. No abstract available.
-
Primary Prevention Ahead of Pregnancy.Dtsch Arztebl Int. 2017 Jul 24;114(29-30):504-505. doi: 10.3238/arztebl.2017.0504b. Dtsch Arztebl Int. 2017. PMID: 28818181 Free PMC article. No abstract available.
References
-
- Britt W, et al. Arvin A, Campadelli-Fiume G, Mocarski E, editors. Virus entry into host, establishment of infection, spread in host, mechanisms of tissue damage. Cambridge: Cambridge University Press. 2007;41:1–88. - PubMed
-
- Ludwig A, Hengel A. Epidemiological impact and disease burden of congenital cytomegalovirus infection in Europe. Eurosurveillance. 2009;14:1–7. - PubMed
-
- Britt W. Controversies in the natural history of congenital human cytomegalovirus infection: the paradox of infection and disease in offspring of women with immunity prior to pregnancy. Med Microbiol Immunol. 2015;204:263–271. - PubMed
-
- Revello MG, Zavattoni M, Furione M, Lilleri D, Gorini G, Gerna G. Diagnosis and outcome of preconceptional and periconceptional primary human cytomegalovirus infections. J Infect Dis. 2002;186:553–557. - PubMed
-
- Enders G, Daiminger A, Bäder U, Exler S, Enders M. Intrauterine transmission and clinical outcome of 248 pregnancies with primary cytomegalovirus infection in relation to gestational age. J Clin Virol. 2011;52:244–246. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical