

Multiple Organ Dysfunction in Children Mechanically Ventilated for Acute Respiratory Failure
- PMID: 28212163
- PMCID: PMC5380520
- DOI: 10.1097/PCC.0000000000001091
Multiple Organ Dysfunction in Children Mechanically Ventilated for Acute Respiratory Failure
Abstract
Objectives: The impact of extrapulmonary organ dysfunction, independent from sepsis and lung injury severity, on outcomes in pediatric acute respiratory failure is unclear. We sought to determine the frequency, timing, and risk factors for extrapulmonary organ dysfunction and the independent association of multiple organ dysfunction syndrome with outcomes in pediatric acute respiratory failure.
Design: Secondary observational analysis of the Randomized Evaluation of Sedation Titration for Respiratory Failure cluster-randomized prospective clinical trial conducted between 2009 and 2013.
Setting: Thirty-one academic PICUs in the United States.
Patients: Two thousand four hundred forty-nine children mechanically ventilated for acute respiratory failure enrolled in Randomized Evaluation of Sedation Titration for Respiratory Failure.
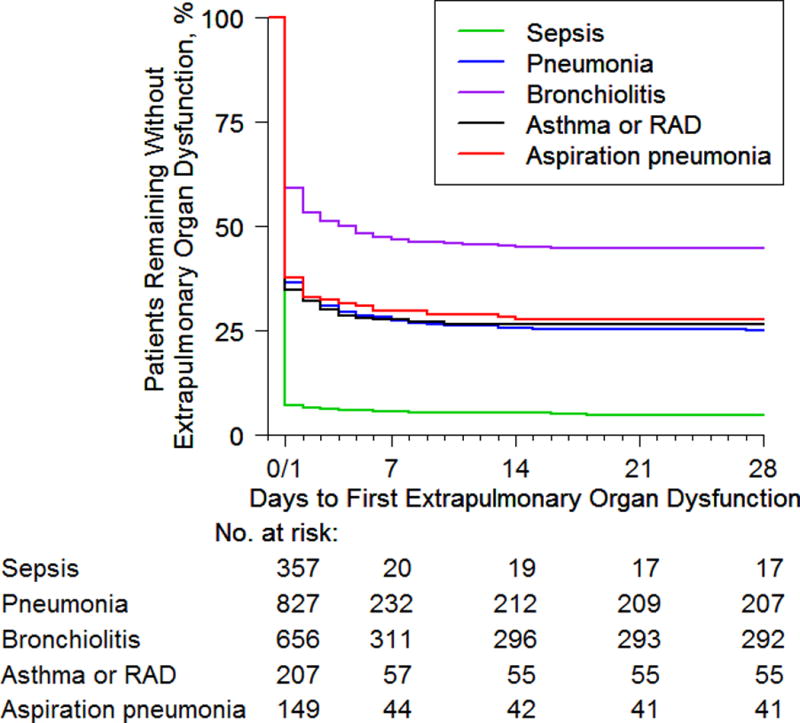
Measurements and main results: Organ dysfunction was defined using criteria published for pediatric sepsis. Multiple organ dysfunction syndrome was defined as respiratory dysfunction one or more extrapulmonary organ dysfunctions. We used multivariable logistic regression to identify risk factors for multiple organ dysfunction syndrome, and logistic or proportional hazards regression to compare clinical outcomes. All analyses accounted for PICU as a cluster variable. Overall, 73% exhibited extrapulmonary organ dysfunction, including 1,547 (63%) with concurrent multiple organ dysfunction syndrome defined by onset on day 0/1 and 244 (10%) with new multiple organ dysfunction syndrome with onset on day 2 or later. Most patients (93%) with indirect lung injury from sepsis presented with concurrent multiple organ dysfunction syndrome, whereas patients with direct lung injury had both concurrent (56%) and new (12%) multiple organ dysfunction syndrome. Risk factors for concurrent multiple organ dysfunction syndrome included older age, illness severity, sepsis, cancer, and moderate/severe lung injury. Risk factors for new multiple organ dysfunction syndrome were moderate/severe lung injury and neuromuscular blockade. Both concurrent and new multiple organ dysfunction syndrome were associated with 90-day in-hospital mortality (concurrent: adjusted odds ratio, 6.54; 95% CI, 3.00-14.25 and new: adjusted odds ratio, 3.21; 95% CI, 1.48-6.93) after adjusting for sepsis, moderate/severe lung injury, and other baseline characteristics.
Conclusions: Extrapulmonary organ dysfunction was common, generally occurred concurrent with respiratory dysfunction (especially in sepsis), and was a major risk factor for mortality in pediatric acute respiratory failure.
Conflict of interest statement
None of the authors have potential conflicts of interest to report.
Figures

Comment in
-
New Insights Into Acute Respiratory Failure and Extrapulmonary Organ Dysfunction.Pediatr Crit Care Med. 2017 Apr;18(4):383-385. doi: 10.1097/PCC.0000000000001109. Pediatr Crit Care Med. 2017. PMID: 28376004 No abstract available.
References
-
- Santschi M, Jouvet P, Leclerc F, et al. Acute lung injury in children: therapeutic practice and feasibility of international clinical trials. Pediatr Crit Care Med. 2010;11(6):681–689. - PubMed
-
- Erickson S, Schibler A, Numa A, et al. Acute lung injury in pediatric intensive care in Australia and New Zealand: a prospective, multicenter, observational study. Pediatr Crit Care Med. 2007;8(4):317–323. - PubMed
-
- Flori HR, Glidden DV, Rutherford GW, et al. Pediatric acute lung injury: prospective evaluation of risk factors associated with mortality. Am J Respir Crit Care Med. 2005;171(9):995–1001. - PubMed
-
- Lopez-Fernandez Y, Azagra AM, de la Oliva P, et al. Pediatric acute lung injury epidemiology and natural history study: incidence and outcome of the acute respiratory distress syndrome in children. Crit Care Med. 2012;40(12):3238–3245. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
