

Decline in infection-related morbidities following drug-mediated reductions in the intensity of Schistosoma infection: A systematic review and meta-analysis
- PMID: 28212414
- PMCID: PMC5333910
- DOI: 10.1371/journal.pntd.0005372
Decline in infection-related morbidities following drug-mediated reductions in the intensity of Schistosoma infection: A systematic review and meta-analysis
Abstract
Background: Since 1984, WHO has endorsed drug treatment to reduce Schistosoma infection and its consequent morbidity. Cross-sectional studies suggest pre-treatment correlation between infection intensity and risk for Schistosoma-related pathology. However, evidence also suggests that post-treatment reduction in intensity may not reverse morbidity because some morbidities occur at all levels of infection, and some reflect permanent tissue damage. The aim of this project was to systematically review evidence on drug-based control of schistosomiasis and to develop a quantitative estimate of the impact of post-treatment reductions in infection intensity on prevalence of infection-associated morbidity.
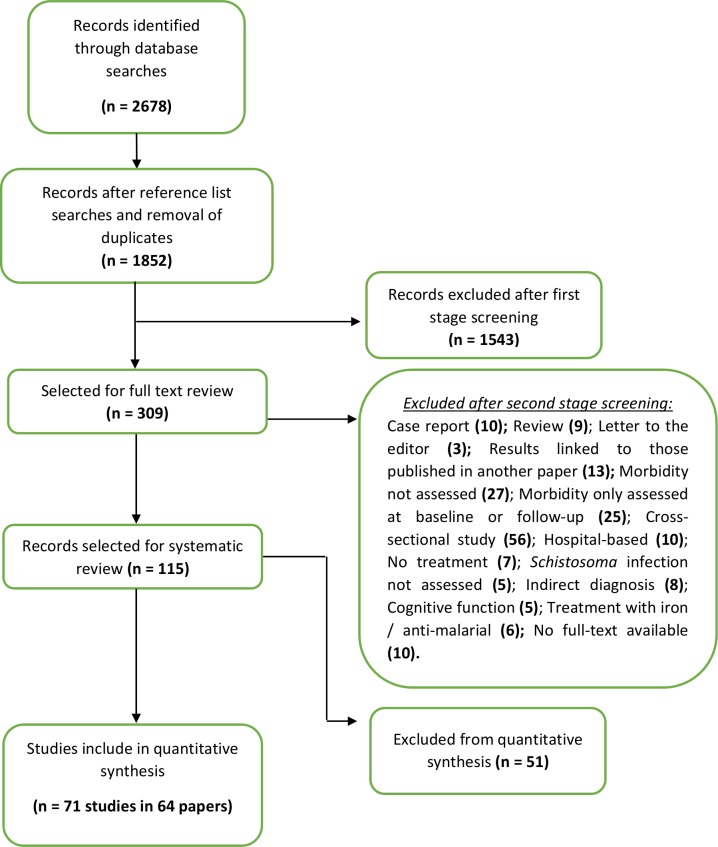
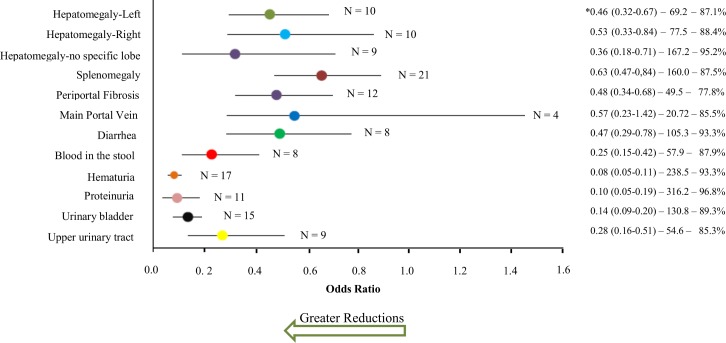
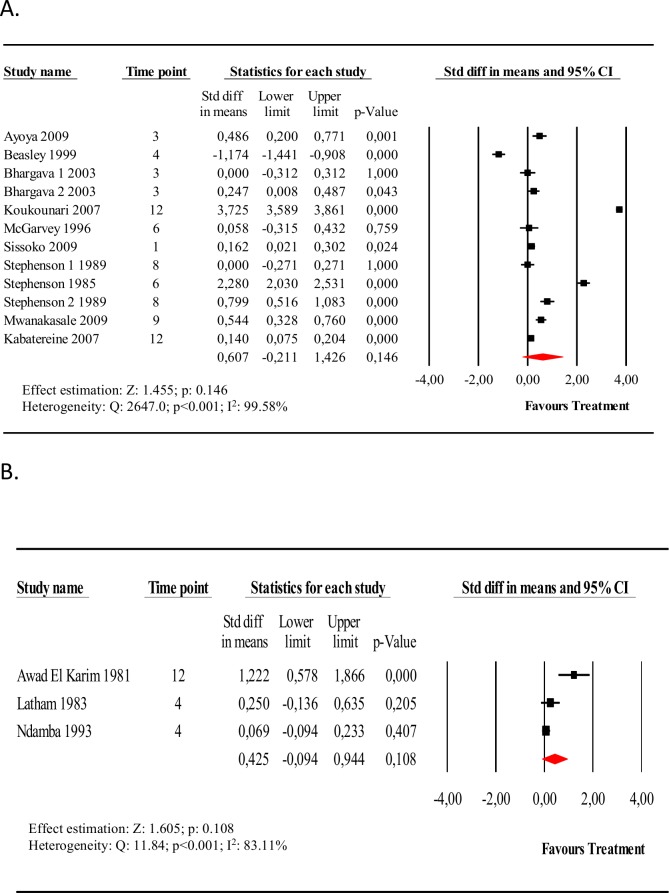
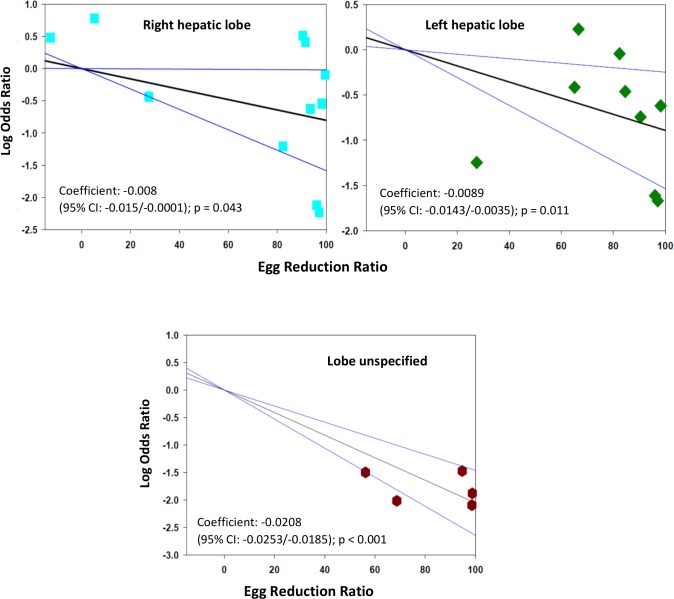
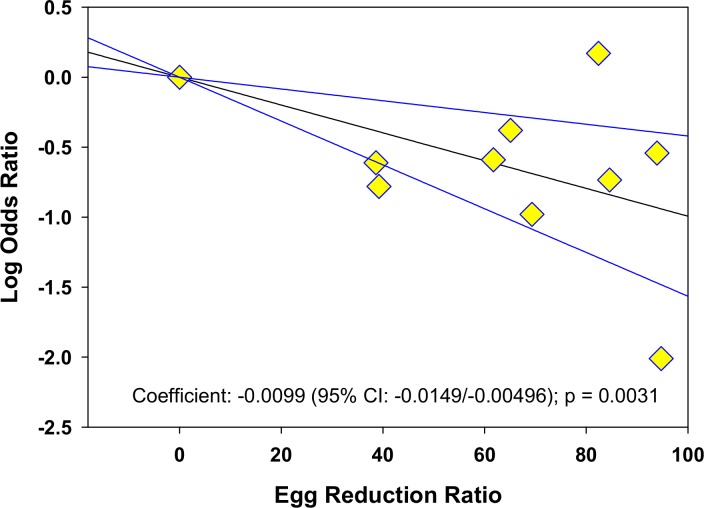
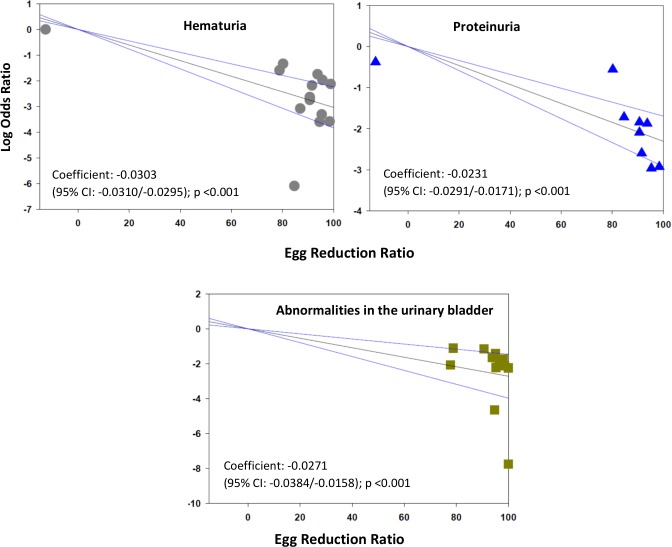
Methodology/principal findings: This review was registered at inception with PROSPERO (CRD42015026080). Studies that evaluated morbidity before and after treatment were identified by online searches and searches of private archives. Post-treatment odds ratios or standardized mean differences were calculated for each outcome, and these were correlated to treatment-related egg count reduction ratios (ERRs) by meta-regression. A greater ERR correlated with greater reduction in odds of most morbidities. Random effects meta-analysis was used to derive summary estimates: after treatment of S. mansoni and S. japonicum, left-sided hepatomegaly was reduced by 54%, right-sided hepatomegaly by 47%, splenomegaly by 37%, periportal fibrosis by 52%, diarrhea by 53%, and blood in stools by 75%. For S. haematobium, hematuria was reduced by 92%, proteinuria by 90%, bladder lesions by 86%, and upper urinary tract lesions by 72%. There were no consistent changes in portal dilation or hemoglobin levels. In sub-group analysis, age, infection status, region, parasite species, and interval to follow-up were associated with meaningful differences in outcome.
Conclusion/significance: While there are challenges to implementing therapy for schistosomiasis, and praziquantel therapy is not fully curative, reductions in egg output are significantly correlated with decreased morbidity and can be used to project diminution in disease burden when contemplating more aggressive strategies to minimize infection intensity.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Booth M, Guyatt HL, Li Y, Tanner M. The morbidity attributable to Schistosoma japonicum infection in 3 villages in Dongting Lake region, Hunan province, PR China. Trop Med Int Health. 1996;1(5):646–654. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
