

Using high-sensitivity sequencing for the detection of mutations in BTK and PLCγ2 genes in cellular and cell-free DNA and correlation with progression in patients treated with BTK inhibitors
- PMID: 28212557
- PMCID: PMC5392298
- DOI: 10.18632/oncotarget.15316
Using high-sensitivity sequencing for the detection of mutations in BTK and PLCγ2 genes in cellular and cell-free DNA and correlation with progression in patients treated with BTK inhibitors
Abstract
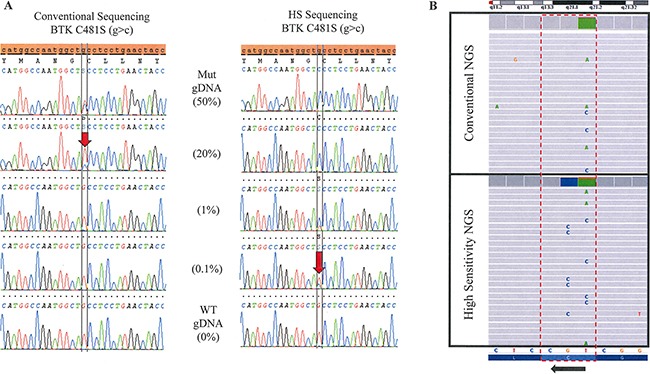
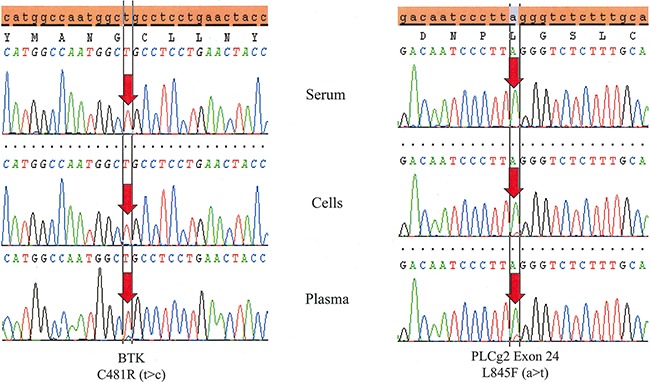
Patients with chronic lymphocytic leukemia (CLL) that develop resistance to Bruton tyrosine kinase (BTK) inhibitors are typically positive for mutations in BTK or phospholipase c gamma 2 (PLCγ2). We developed a high sensitivity (HS) assay utilizing wild-type blocking polymerase chain reaction achieved via bridged and locked nucleic acids. We used this high sensitivity assay in combination with Sanger sequencing and next generation sequencing (NGS) and tested cellular DNA and cell-free DNA (cfDNA) from patients with CLL treated with the BTK inhibitor, ibrutinib. We also tested ibrutinib-naïve patients with CLL. HS testing achieved 100x greater sensitivity than Sanger. HS Sanger sequencing was capable of detecting < 1 mutant allele in background of 1000 wild-type alleles (1:1000). Similar sensitivity was achieved with HS NGS. No BTK or PLCγ2 mutations were detected in any of the 44 ibrutinib-naïve CLL patients. We demonstrate that without the HS testing 56% of positive samples would have been missed for BTK and 85% of PLCγ2 would have been missed. With the use of HS, we were able to detect multiple mutant clones in the same sample in 37.5% of patients; most would have been missed without HS testing. We also demonstrate that with HS sequencing, plasma cfDNA is more reliable than cellular DNA in detecting mutations. Our studies indicate that wild-type blocking and HS sequencing is necessary for proper and early detection of BTK or PLCγ2 mutations in monitoring patients treated with BTK inhibitors. Furthermore, cfDNA from plasma is very reliable sample-type for testing.
Keywords: BTK; CLL; PLCγ2; ibrutinib; resistance.
Conflict of interest statement
Adam Albitar, Wanlong Ma, Ivan DeDios, Jeffrey Estella, and Maher Albitar: Work for a diagnostic company offering testing for BTK and PLCγ2. Adrian Wiestner: Receives research funding from PCYC.
Figures
References
-
- Farooqui MZ, Valdez J, Martyr S, Aue G, Saba N, Niemann CU, Herman SE, Tian X, Marti G, Soto S, Hughes TE, Jones J, Lipsky A, et al. Ibrutinib for previously untreated and relapsed or refractory chronic lymphocytic leukaemia with TP53 aberrations: a phase 2, single-arm trial. Lancet Oncol. 2015;16:169–76. - PMC - PubMed
-
- Byrd JC, Furman RR, Coutre SE, Burger JA, Blum KA, Coleman M, Wierda WG, Jones JA, Zhao W, Heerema NA, Johnson AJ, Shaw Y, Bilotti E, Zhou C, et al. Three-year follow-up of treatment-naive and previously treated patients with CLL and SLL receiving single-agent ibrutinib. Blood. 2015:blood–2014. - PMC - PubMed
-
- Advani RH, Buggy JJ, Sharman JP, Smith SM, Boyd TE, Grant B, Kolibaba KS, Furman RR, Rodriguez S, Chang BY, Sukbuntherng J, Izumi R, Hamdy A, et al. Bruton tyrosine kinase inhibitor ibrutinib (PCI-32765) has significant activity in patients with relapsed/refractory B-cell malignancies. J Clin Oncol. 2013;31:88–94. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
