

Health State Preference Weights for the Glasgow Outcome Scale Following Traumatic Brain Injury: A Systematic Review and Mapping Study
- PMID: 28212955
- PMCID: PMC5339086
- DOI: 10.1016/j.jval.2016.09.2398
Health State Preference Weights for the Glasgow Outcome Scale Following Traumatic Brain Injury: A Systematic Review and Mapping Study
Abstract
Background: Valid and relevant estimates of health state preference weights (HSPWs) for Glasgow Outcome Scale (GOS) categories are a key input of economic models evaluating treatments for traumatic brain injury (TBI).
Objectives: To characterize existing HSPW estimates, and model the EuroQol five-dimensional questionnaire (EQ-5D) from the GOS, to inform parameterization of future economic models.
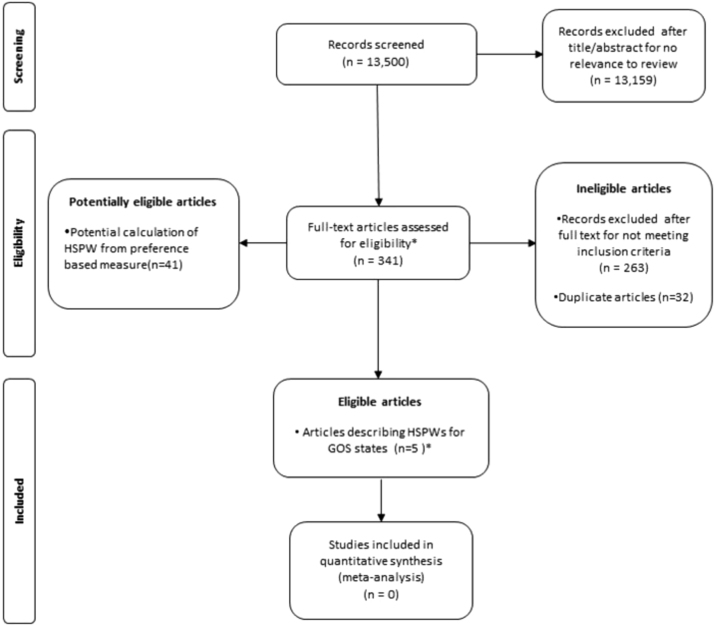
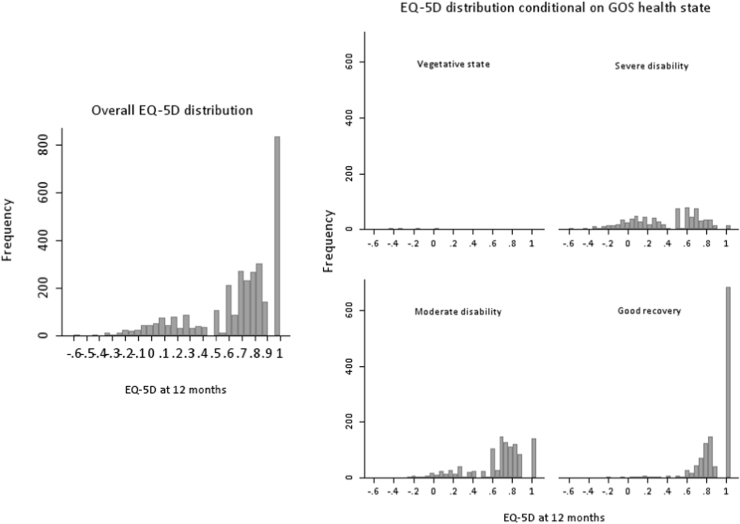
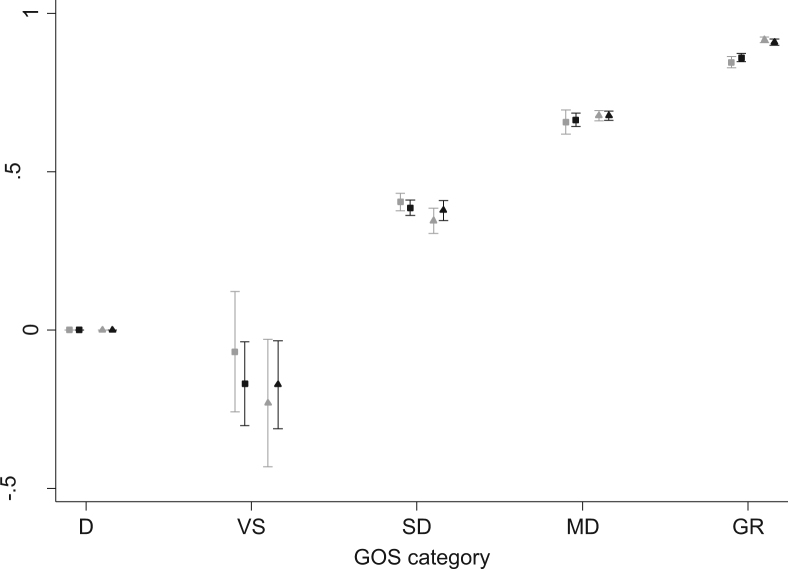
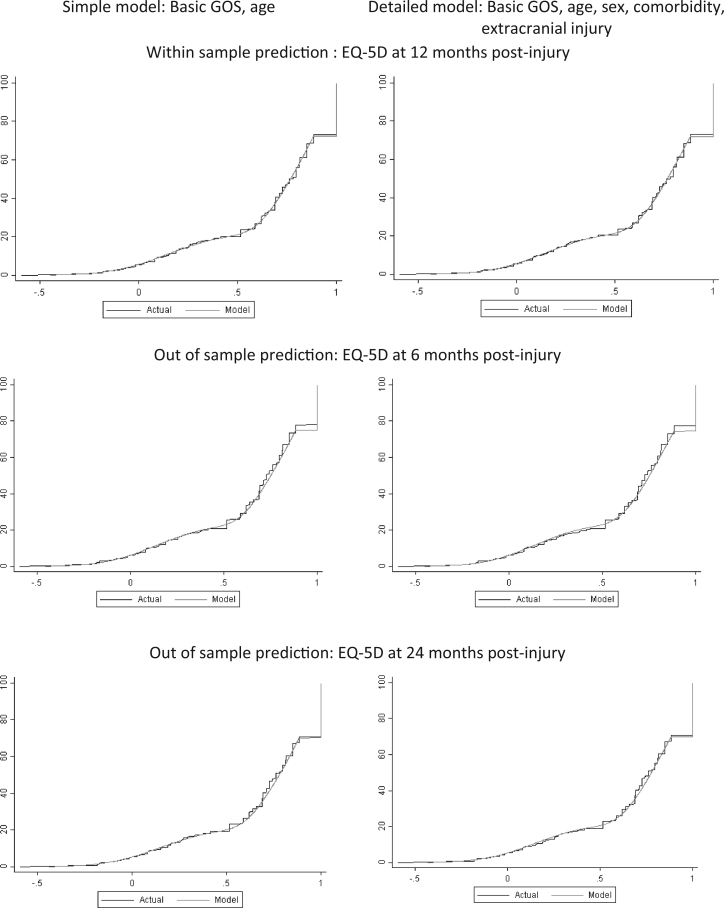
Methods: A systematic review of HSPWs for GOS categories following TBI was conducted using a highly sensitive search strategy implemented in an extensive range of information sources between 1975 and 2016. A cross-sectional mapping study of GOS health states onto the three-level EQ-5D UK tariff index values was also performed in patients with significant TBI (head region Abbreviated Injury Scale score ≥3) from the Victoria State Trauma Registry. A limited dependent variable mixture model was used to estimate the 12-month EQ-5D UK value set as a function of GOS category, age, and other explanatory variables.
Results: Six unique HSPWs from five eligible studies were identified. All studies were at high risk of bias with limited applicability. The magnitude of HSPWs differed significantly between studies. Three class mixture models demonstrated excellent goodness of fit to the observed Victoria State Trauma Registry data. GOS category, age at injury, sex, comorbidity, and major extracranial injury all had significant independent effects on mean EQ-5D utility values.
Conclusions: The few available HSPWs for GOS categories are challenged by potential biases and restricted generalizability. Mixture models are presented to provide HSPWs for GOS categories consistent with the National Institute for Health and Care Excellence reference case.
Keywords: EuroQol-5D; Glasgow Outcome Scale; craniocerebral trauma; decision analysis models; economic models; health status indicators; mapping study; quality of life; quality-adjusted life-years; systematic review.
Copyright © 2017 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Drummond M.F. Evaluation of Health Care Programmes. 3rd ed. Oxford University Press; Oxford, UK: 2005. Methods for the Economic.
-
- Weinstein M.C., Torrance G., McGuire A. QALYs: the basics. Value Health. 2009;12(Suppl. 1):S5–S9. - PubMed
-
- Petrou S., Gray A. Economic evaluation using decision analytical modelling: design, conduct, analysis, and reporting. BMJ. 2011;342:d1766. - PubMed
-
- Tolley K. Hayward Medical Communications; 2009. What Are Health Utilities? London.
-
- Papaioannou D., Brazier J.E., Paisley S. NICE DSU Technical Support Document 9. National Institute for Health and Care Excellence; London: 2011. The Identification, Review and Synthesis of Health State Utility Values from the Literature. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
