

Costs and Outcomes of Increasing Access to Bariatric Surgery: Cohort Study and Cost-Effectiveness Analysis Using Electronic Health Records
- PMID: 28212974
- PMCID: PMC5338873
- DOI: 10.1016/j.jval.2016.08.734
Costs and Outcomes of Increasing Access to Bariatric Surgery: Cohort Study and Cost-Effectiveness Analysis Using Electronic Health Records
Abstract
Objectives: To estimate costs and outcomes of increasing access to bariatric surgery in obese adults and in population subgroups of age, sex, deprivation, comorbidity, and obesity category.
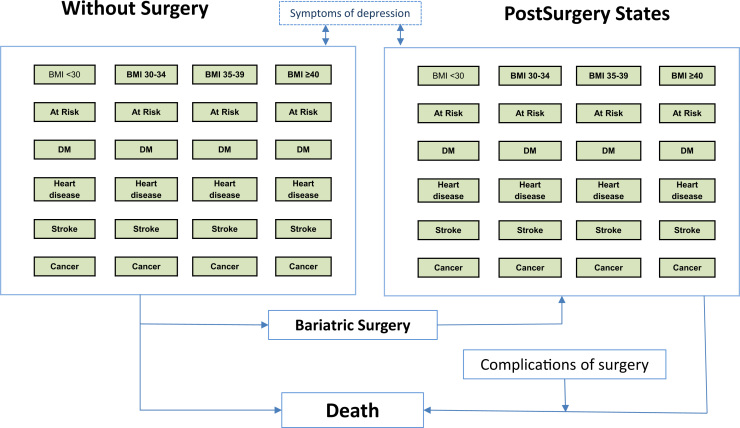
Methods: A cohort study was conducted using primary care electronic health records, with linked hospital utilization data, for 3,045 participants who underwent bariatric surgery and 247,537 participants who did not undergo bariatric surgery. Epidemiological analyses informed a probabilistic Markov model to compare bariatric surgery, including equal proportions with adjustable gastric banding, gastric bypass, and sleeve gastrectomy, with standard nonsurgical management of obesity. Outcomes were quality-adjusted life-years (QALYs) and net monetary benefits at a threshold of £30,000 per QALY.
Results: In a UK population of 250,000 adults, there may be 7,163 people with morbid obesity including 1,406 with diabetes. The immediate cost of 1,000 bariatric surgical procedures is £9.16 million, with incremental discounted lifetime health care costs of £15.26 million (95% confidence interval £15.18-£15.36 million). Patient-years with diabetes mellitus will decrease by 8,320 (range 8,123-8,502). Incremental QALYs will increase by 2,142 (range 2,032-2,256). The estimated cost per QALY gained is £7,129 (range £6,775-£7,506). Net monetary benefits will be £49.02 million (range £45.72-£52.41 million). Estimates are similar for subgroups of age, sex, and deprivation. Bariatric surgery remains cost-effective if the procedure is twice as costly, or if intervention effect declines over time.
Conclusions: Diverse obese individuals may benefit from bariatric surgery at acceptable cost. Bariatric surgery is not cost-saving, but increased health care costs are exceeded by health benefits to obese individuals.
Keywords: bariatric surgery; cost-effectiveness analysis; diabetes mellitus; obesity.
Copyright © 2017 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Romero-Corral A., Montori V.M., Somers V.K. Association of bodyweight with total mortality and with cardiovascular events in coronary artery disease: a systematic review of cohort studies. Lancet. 2006;368:666–678. - PubMed
-
- Sjöström L., Narbro K., Sjöström C.D. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741–752. - PubMed
-
- Booth H., Khan O., Prevost T. Incidence of type 2 diabetes after bariatric surgery: population-based matched cohort study. Lancet Diabetes Endocrinol. 2014;2:963–968. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
