

Effects of Dopamine Donor Pretreatment on Graft Survival after Kidney Transplantation: A Randomized Trial
- PMID: 28213388
- PMCID: PMC5338714
- DOI: 10.2215/CJN.07600716
Effects of Dopamine Donor Pretreatment on Graft Survival after Kidney Transplantation: A Randomized Trial
Abstract
Background and objectives: Donor dopamine improves initial graft function after kidney transplantation due to antioxidant properties. We investigated if a 4 µg/kg per minute continuous dopamine infusion administered after brain-death confirmation affects long-term graft survival and examined the exposure-response relationship with treatment duration.
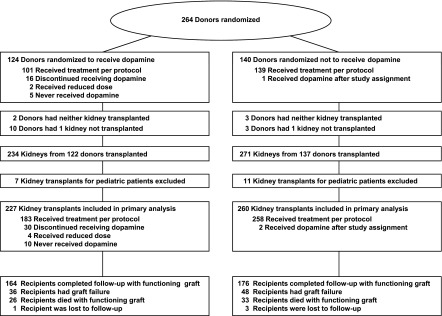
Design, setting, participants, & measurements: Five-year follow-up of 487 renal transplant patients from 60 European centers who had participated in the randomized, multicenter trial of dopamine donor pretreatment between 2004 and 2007 (ClinicalTrials.gov identifier: NCT00115115).
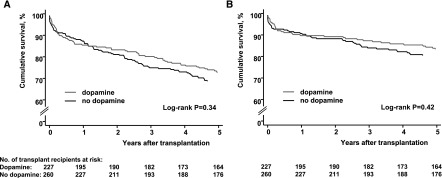
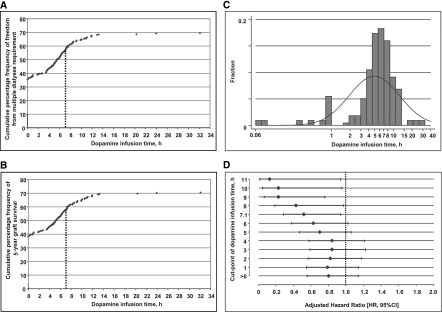
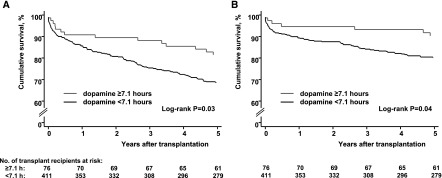
Results: Follow-up was complete in 99.2%. Graft survival was 72.6% versus 68.7% (P=0.34), and 83.3% versus 80.4% (P=0.42) after death-censoring in treatment and control arms according to trial assignment. Although infusion times varied substantially in the treatment arm (range 0-32.2 hours), duration of the dopamine infusion and all-cause graft failure exhibited an exposure-response relationship (hazard ratio, 0.96; 95% confidence interval [95% CI], 0.92 to 1.00, per hour). Cumulative frequency curves of graft survival and exposure time of the dopamine infusion indicated a maximum response rate at 7.10 hours (95% CI, 6.99 to 7.21), which almost coincided with the optimum infusion time for improvement of early graft function (7.05 hours; 95% CI, 6.92 to 7.18). Taking infusion time of 7.1 hours as threshold in subsequent graft survival analyses indicated a relevant benefit: Overall, 81.5% versus 68.5%; P=0.03; and 90.3% versus 80.2%; P=0.04 after death-censoring.
Conclusions: We failed to show a significant graft survival advantage on intention-to-treat. Dopamine infusion time was very short in a considerable number of donors assigned to treatment. Our finding of a significant, nonlinear exposure-response relationship disclosed a threshold value of the dopamine infusion time that may improve long-term kidney graft survival.
Keywords: arm; brain; brain death; brain-dead donor; cadaver organ transplantation; confidence intervals; death; donor pretreatment; dopamine; follow-up studies; graft survival; humans; intention to treat analysis; ischemia-reperfusion; kidney transplantation; outcomes; renal protection; renal transplantation; survival analysis; tissue donors; transplants.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Optimizing Graft Survival by Pretreatment of the Donor.Clin J Am Soc Nephrol. 2017 Mar 7;12(3):388-390. doi: 10.2215/CJN.00900117. Epub 2017 Feb 17. Clin J Am Soc Nephrol. 2017. PMID: 28213389 Free PMC article. No abstract available.
References
-
- Rosendale JD, Kauffman HM, McBride MA, Chabalewski FL, Zaroff JG, Garrity ER, Delmonico FL, Rosengard BR: Aggressive pharmacologic donor management results in more transplanted organs. Transplantation 75: 482–487, 2003 - PubMed
-
- Novitzky D, Cooper DK, Rosendale JD, Kauffman HM: Hormonal therapy of the brain-dead organ donor: Experimental and clinical studies. Transplantation 82: 1396–1401, 2006 - PubMed
-
- Malinoski DJ, Patel MS, Ahmed O, Daly MC, Mooney S, Graybill CO, Foster CE, Salim A; United Network for Organ Sharing (UNOS) Region 5 Donor Management Goals (DMG) Workgroup : The impact of meeting donor management goals on the development of delayed graft function in kidney transplant recipients. Am J Transplant 13: 993–1000, 2013 - PubMed
-
- Wood KE, Becker BN, McCartney JG, D’Alessandro AM, Coursin DB: Care of the potential organ donor. N Engl J Med 351: 2730–2739, 2004 - PubMed
-
- Kainz A, Wilflingseder J, Mitterbauer C, Haller M, Burghuber C, Perco P, Langer RM, Heinze G, Oberbauer R: Steroid pretreatment of organ donors to prevent postischemic renal allograft failure: A randomized, controlled trial. Ann Intern Med 153: 222–230, 2010 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
