

Caesarean sections and for-profit status of hospitals: systematic review and meta-analysis
- PMID: 28213600
- PMCID: PMC5318567
- DOI: 10.1136/bmjopen-2016-013670
Caesarean sections and for-profit status of hospitals: systematic review and meta-analysis
Abstract
Objective: Financial incentives may encourage private for-profit providers to perform more caesarean section (CS) than non-profit hospitals. We therefore sought to determine the association of for-profit status of hospital and odds of CS.
Design: Systematic review and meta-analysis.
Data sources: MEDLINE, EMBASE and the Cochrane Database of Systematic Reviews from the first year of records through February 2016.
Eligibility criteria: To be eligible, studies had to report data to allow the calculation of ORs of CS comparing private for-profit hospitals with public or private non-profit hospitals in a specific geographic area.
Outcomes: The prespecified primary outcome was the adjusted OR of births delivered by CS in private for-profit hospitals as compared with public or private non-profit hospitals; the prespecified secondary outcome was the crude OR of CS in private for-profit hospitals as compared with public or private non-profit hospitals.
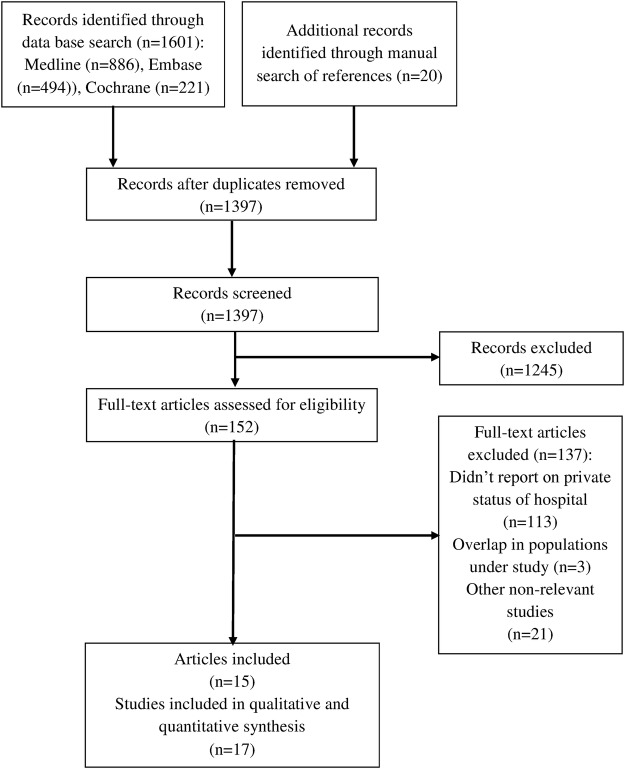
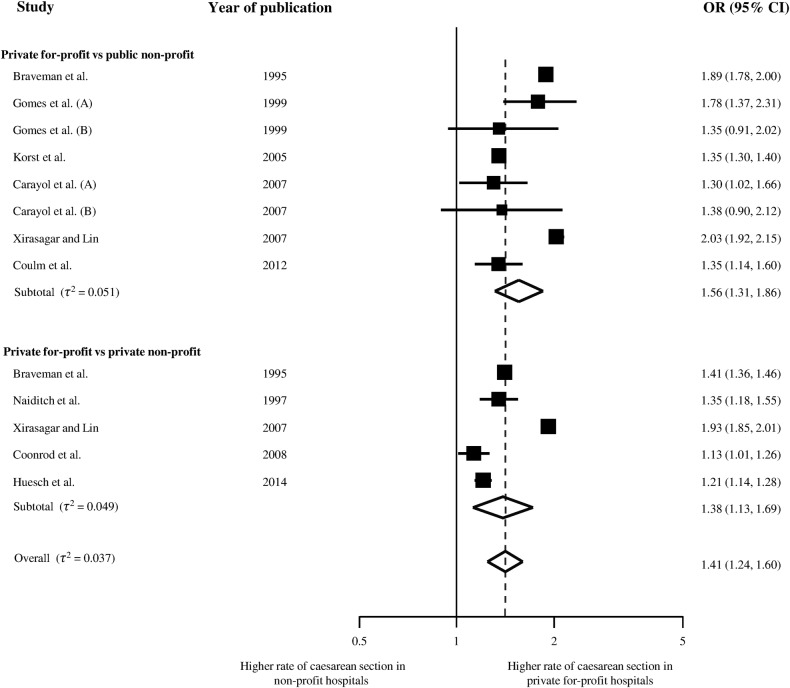
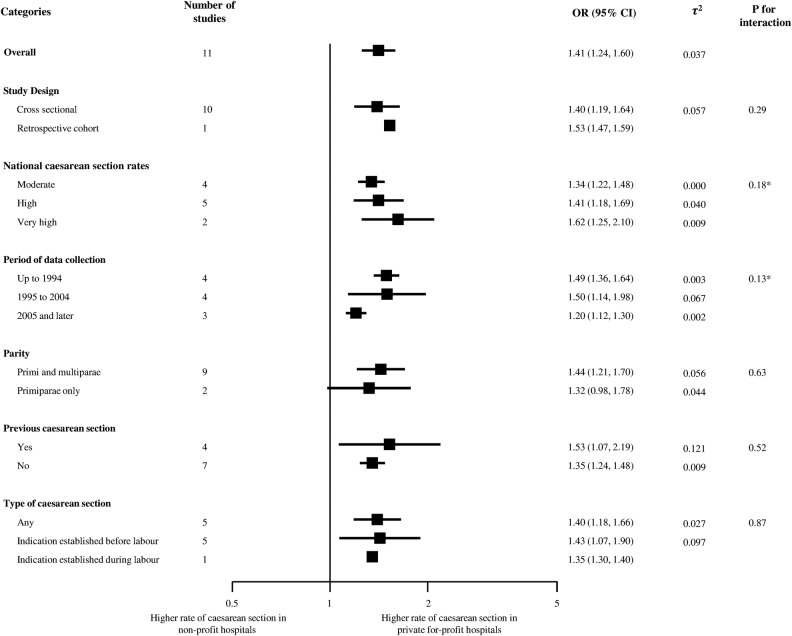
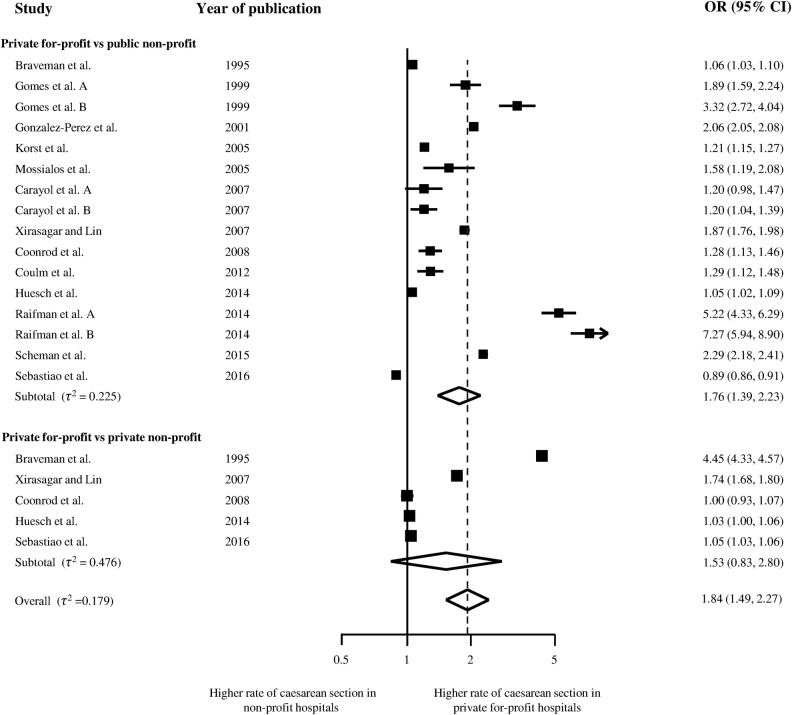
Results: 15 articles describing 17 separate studies in 4.1 million women were included. In a meta-analysis of 11 studies, the adjusted odds of delivery by CS was 1.41 higher in for-profit hospitals as compared with non-profit hospitals (95% CI 1.24 to 1.60) with no relevant heterogeneity between studies (τ2≤0.037). Findings were robust across subgroups of studies in stratified analyses. The meta-analysis of crude estimates from 16 studies revealed a somewhat more pronounced association (pooled OR 1.84, 95% CI 1.49 to 2.27) with moderate-to-high heterogeneity between studies (τ2≥0.179).
Conclusions: CS are more likely to be performed by for-profit hospitals as compared with non-profit hospitals. This holds true regardless of women's risk and contextual factors such as country, year or study design. Since financial incentives are likely to play an important role, we recommend examination of incentive structures of for-profit hospitals to identify strategies that encourage appropriate provision of CS.
Keywords: caesarean section; financial incentives; for-profit hospital; health services; medical practice variation; non-profit hospital.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures
References
-
- Stephenson PA, Bakoula C, Hemminki E et al. Patterns of use of obstetrical interventions in 12 countries. Paediatr Perinat Epidemiol 1993;7:45–54. doi:10.1111/j.1365-3016.1993.tb00600.x - DOI - PubMed
-
- Hoxha I, Busato A, Luta X. Medical practice variations in reproductive, obstetric, and gynaecological care. In: Johnson A, Stukel T, eds. Medical practice variations. Health services research series. New York, NY: Springer, 2015:141–60.
-
- Main EK, Morton CH, Melsop K et al. Creating a public agenda for maternity safety and quality in cesarean delivery. Obstet Gynecol 2012;120:1194–8. doi:http://10.1097/AOG.0b013e31826fc13d - DOI - PubMed
-
- OECD. Health at a glance 2011L OECD indicators. OECD Publishing, 2011.
-
- Molina G, Weiser TG, Lipsitz SR et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. JAMA 2015;314:2263–70. doi:10.1001/jama.2015.15553 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical