

Educating religious leaders to promote uptake of male circumcision in Tanzania: a cluster randomised trial
- PMID: 28214093
- PMCID: PMC5364327
- DOI: 10.1016/S0140-6736(16)32055-4
Educating religious leaders to promote uptake of male circumcision in Tanzania: a cluster randomised trial
Abstract
Background: Male circumcision is being widely deployed as an HIV prevention strategy in countries with high HIV incidence, but its uptake in sub-Saharan Africa has been below targets. We did a study to establish whether educating religious leaders about male circumcision would increase uptake in their village.
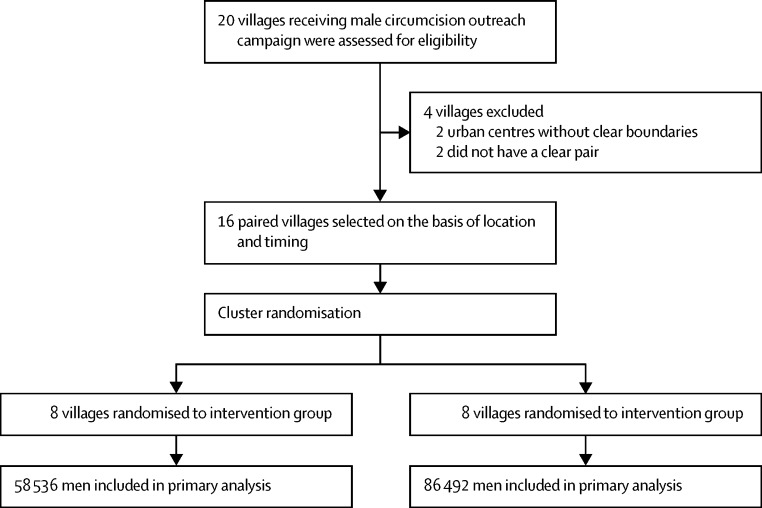
Methods: In this cluster randomised trial in northwest Tanzania, eligible villages were paired by proximity (<60 km) and the time that a free male circumcision outreach campaign from the Tanzanian Ministry of Health became available in their village. All villages received the standard male circumcision outreach activities provided by the Ministry of Health. Within the village pairs, villages were randomly assigned by coin toss to receive either additional education for Christian church leaders on scientific, religious, and cultural aspects of male circumcision (intervention group), or standard outreach only (control group). Church leaders or their congregations were not masked to random assignment. The educational intervention consisted of a 1-day seminar co-taught by a Tanzanian pastor and a Tanzanian clinician who worked with the Ministry of Health, and meetings with the study team every 2 weeks thereafter, for the duration of the circumcision campaign. The primary outcome was the proportion of male individuals in a village who were circumcised during the campaign, using an intention-to-treat analysis that included all men in the village. This trial is registered with ClinicalTrials.gov, number NCT 02167776.
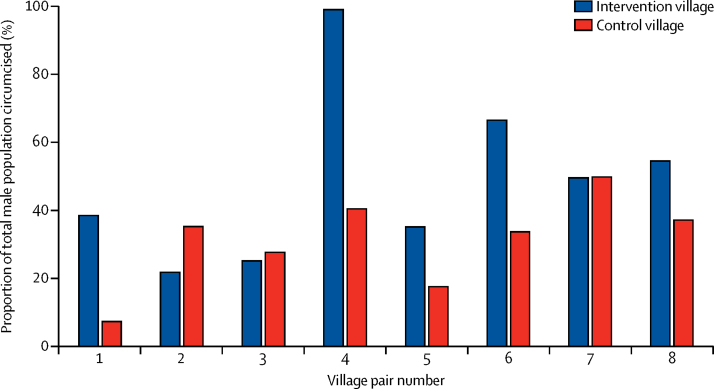
Findings: Between June 15, 2014, and Dec 10, 2015, we provided education for church leaders in eight intervention villages and compared the outcomes with those in eight control villages. In the intervention villages, 52·8% (30 889 of 58 536) of men were circumcised compared with 29·5% (25 484 of 86 492) of men in the eight control villages (odds ratio 3·2 [95% CI, 1·4-7·3]; p=0·006).
Interpretation: Education of religious leaders had a substantial effect on uptake of male circumcision, and should be considered as part of male circumcision programmes in other sub-Saharan African countries. This study was conducted in one region in Tanzania; however, we believe that our intervention is generalisable. We equipped church leaders with knowledge and tools, and ultimately each leader established the most culturally-appropriate way to promote male circumcision. Therefore, we think that the process of working through religious leaders can serve as an innovative model to promote healthy behaviour, leading to HIV prevention and other clinically relevant outcomes, in a variety of settings.
Funding: Bill & Melinda Gates Foundation, National Institutes of Health, and the Mulago Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Educating religious leaders to create demand for medical male circumcision.Lancet. 2017 Mar 18;389(10074):1080-1082. doi: 10.1016/S0140-6736(17)30318-5. Epub 2017 Feb 15. Lancet. 2017. PMID: 28214094 Free PMC article. No abstract available.
Similar articles
-
The Spear and Shield intervention to increase the availability and acceptability of voluntary medical male circumcision in Zambia: a cluster randomised controlled trial.Lancet HIV. 2015 May;2(5):e181-9. doi: 10.1016/S2352-3018(15)00042-9. Lancet HIV. 2015. PMID: 26120594 Free PMC article. Clinical Trial.
-
Population uptake of HIV testing, treatment, viral suppression, and male circumcision following a community-based intervention in Botswana (Ya Tsie/BCPP): a cluster-randomised trial.Lancet HIV. 2020 Jun;7(6):e422-e433. doi: 10.1016/S2352-3018(20)30103-X. Lancet HIV. 2020. PMID: 32504575 Free PMC article. Clinical Trial.
-
Improving risk perception and uptake of voluntary medical male circumcision with peer-education sessions and incentives, in Manicaland, East Zimbabwe: study protocol for a pilot randomised trial.Trials. 2020 Jan 23;21(1):108. doi: 10.1186/s13063-020-4048-2. Trials. 2020. PMID: 31973744 Free PMC article.
-
The effectiveness of demand creation interventions for voluntary male medical circumcision for HIV prevention in sub-Saharan Africa: a mixed methods systematic review.J Int AIDS Soc. 2019 Jul;22 Suppl 4(Suppl Suppl 4):e25299. doi: 10.1002/jia2.25299. J Int AIDS Soc. 2019. PMID: 31328419 Free PMC article.
-
Acceptability of male circumcision for prevention of HIV/AIDS in sub-Saharan Africa: a review.AIDS Behav. 2007 May;11(3):341-55. doi: 10.1007/s10461-006-9169-4. Epub 2006 Oct 20. AIDS Behav. 2007. PMID: 17053855 Free PMC article. Review.
Cited by
-
Embracing challenging complexity: exploring handwashing behavior from a combined socioecological and intersectional perspective in Sierra Leone.BMC Public Health. 2021 Oct 14;21(1):1857. doi: 10.1186/s12889-021-11923-1. BMC Public Health. 2021. PMID: 34649535 Free PMC article.
-
Conceptual model for pluralistic healthcare behaviour: results from a qualitative study in southwestern Uganda.BMJ Open. 2020 Apr 20;10(4):e033410. doi: 10.1136/bmjopen-2019-033410. BMJ Open. 2020. PMID: 32317259 Free PMC article.
-
Messaging Circumstances and Economic Pressures as Influences on Linkage to Medical Male Circumcision following Community-Based HIV Testing for Men in Rural Southwest Uganda: A Qualitative Study.AIDS Res Treat. 2018 May 3;2018:8387436. doi: 10.1155/2018/8387436. eCollection 2018. AIDS Res Treat. 2018. PMID: 29854445 Free PMC article.
-
Religious Leaders as Trusted Messengers in Combatting Hypertension in Rural Tanzanian Communities.Am J Hypertens. 2021 Oct 27;34(10):1042-1048. doi: 10.1093/ajh/hpab080. Am J Hypertens. 2021. PMID: 34022044 Free PMC article.
-
Barriers and Facilitators to, and Experience of, Voluntary Medical Male Circumcision Among Men Who Have Sex with Men in China: A Mixed-Methods Study.Arch Sex Behav. 2023 Jul;52(5):2065-2081. doi: 10.1007/s10508-023-02634-2. Epub 2023 Jun 9. Arch Sex Behav. 2023. PMID: 37296334 Free PMC article. Clinical Trial.
References
-
- Bailey RC, Moses S, Parker CB. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet. 2007;369:643–656. - PubMed
-
- Gray RH, Kigozi G, Serwadda D. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet. 2007;369:657–666. - PubMed
-
- WHO Male circumcision for HIV Prevention. HIV/AIDS. Geneva: World Health Organization. http://www.who.int/hiv/topics/malecircumcision/en/ (accessed May 5, 2016).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
