

Systemic thrombolysis increases hemorrhagic stroke risk without survival benefit compared with catheter-directed intervention for the treatment of acute pulmonary embolism
- PMID: 28214483
- PMCID: PMC5324829
- DOI: 10.1016/j.jvsv.2016.11.005
Systemic thrombolysis increases hemorrhagic stroke risk without survival benefit compared with catheter-directed intervention for the treatment of acute pulmonary embolism
Abstract
Background: Systemic thrombolysis (ST) and catheter-directed intervention (CDI) are both used in the treatment of acute pulmonary embolism (PE), but the comparative outcomes of these two therapies remain unclear. The objective of this study was to compare short-term mortality and safety outcomes between the two treatments using a large national database.
Methods: Patients presenting with acute PE were identified in the National Inpatient Sample (NIS) from 2009 to 2012. Comorbidities, clinical characteristics, and invasive procedures were identified using International Classification of Diseases, Ninth Revision (ICD) codes and the Elixhauser comorbidity index. To adjust for anticipated baseline differences between the two treatment groups, propensity score matching was used to create a matched ST cohort with clinical and comorbid characteristics similar to those of the CDI cohort. Subgroups of patients with and without hemodynamic shock were analyzed separately. Primary outcomes were in-hospital mortality, overall bleeding risk, and hemorrhagic stroke risk.
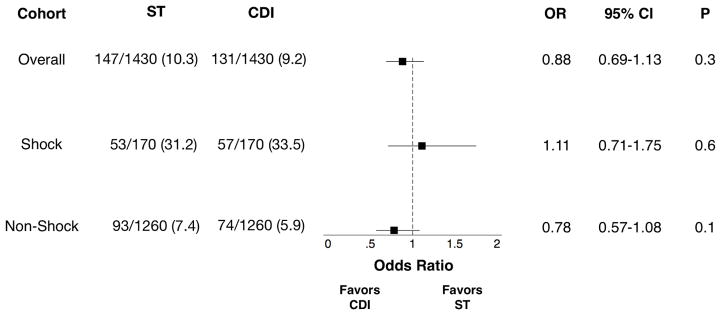
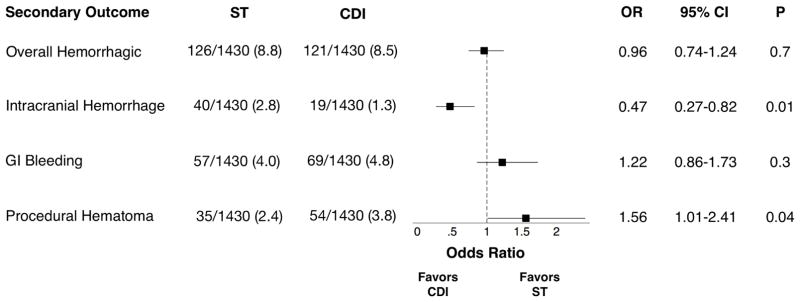
Results: Of 263,955 subjects with acute PE, 1.63% (n = 4272) received ST and 0.55% (n = 1455) received CDI. ST subjects were older, had more chronic comorbidities, and had higher rates of respiratory failure (ST, 27.9% [n = 1192]; CDI, 21.2% [n = 308]; P < .001) and shock (ST, 18.2% [n = 779]; CDI, 12% [n = 174]; P < .001). CDI subjects had higher rates of concurrent deep venous thrombosis (ST, 35.8% [n = 1530]; CDI, 45.9% [n = 668]; P < .001) and vena cava filter placement (ST, 31.1% [n = 1328]; CDI, 57% [n = 830]; P < .001). In the unmatched cohort, ST subjects had higher in-hospital mortality (ST, 16.7% [n = 714]; CDI, 9.4% [n = 136]; P < .001) and hemorrhagic stroke rates (ST, 2.2% [n = 96]; CDI, 1.4% [n = 20]; P = .041). After propensity matching, 1430 patients remained in each cohort; baseline characteristics of the matched cohorts did not differ significantly using standardized difference comparisons. Analysis of the matched cohorts did not demonstrate a significant effect of CDI on in-hospital mortality or overall bleeding risk but did show a significant protective effect against hemorrhagic stroke compared with ST (odds ratio, 0.47; 95% confidence interval, 0.27-0.82; P = .01). Subgroup analysis showed decreased odds of hemorrhagic stroke for CDI in the nonshock subgroup and increased procedural bleeding for CDI but no difference in hemorrhagic stroke risk in the shock subgroup.
Conclusions: ST for acute PE may not improve in-hospital mortality compared with CDI but increases the overall risk of hemorrhagic stroke compared with CDI. Further prospective studies should examine the comparative effectiveness and safety of these two treatments.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Catheter-directed interventions compared with systemic thrombolysis achieve improved ventricular function recovery at a potentially lower complication rate for acute pulmonary embolism.J Vasc Surg Venous Lymphat Disord. 2018 Jul;6(4):425-432. doi: 10.1016/j.jvsv.2017.12.058. Epub 2018 Mar 31. J Vasc Surg Venous Lymphat Disord. 2018. PMID: 29615372 Free PMC article.
-
Outcomes of catheter-directed versus systemic thrombolysis for the treatment of pulmonary embolism: A real-world analysis of national administrative claims.Vasc Med. 2020 Aug;25(4):334-340. doi: 10.1177/1358863X20903371. Epub 2020 Apr 27. Vasc Med. 2020. PMID: 32338580
-
Impact of Inferior Vena Cava Filter Placement on Short-Term Outcomes in Patients with Acute Pulmonary Embolism.Ann Vasc Surg. 2017 Jul;42:71-77. doi: 10.1016/j.avsg.2016.11.015. Epub 2017 Mar 23. Ann Vasc Surg. 2017. PMID: 28341513 Free PMC article.
-
Surgical pulmonary embolectomy and catheter-based therapies for acute pulmonary embolism: A contemporary systematic review.J Thorac Cardiovasc Surg. 2018 Dec;156(6):2155-2167. doi: 10.1016/j.jtcvs.2018.05.085. Epub 2018 Jun 8. J Thorac Cardiovasc Surg. 2018. PMID: 30005883
-
Controversies in the Management of Life-Threatening Pulmonary Embolism.Semin Respir Crit Care Med. 2015 Dec;36(6):835-41. doi: 10.1055/s-0035-1564733. Epub 2015 Nov 23. Semin Respir Crit Care Med. 2015. PMID: 26595043 Review.
Cited by
-
"Hospital survival of patients with pulmonary embolism in a country with limited resources case of the city of Kinshasa".BMC Cardiovasc Disord. 2023 Sep 4;23(1):439. doi: 10.1186/s12872-023-03467-6. BMC Cardiovasc Disord. 2023. PMID: 37667172 Free PMC article.
-
Treatment of high- and intermediate-risk pulmonary embolism using the AngioJet percutaneous mechanical thrombectomy system in patients with contraindications for thrombolytic treatment - a pilot study.Wideochir Inne Tech Maloinwazyjne. 2018 Jun;13(2):233-242. doi: 10.5114/wiitm.2018.75848. Epub 2018 May 16. Wideochir Inne Tech Maloinwazyjne. 2018. PMID: 30002757 Free PMC article.
-
Outcomes of catheter-directed thrombolysis vs. standard medical therapy in patients with acute submassive pulmonary embolism.Pulm Circ. 2020 Apr 8;10(1):2045894019898368. doi: 10.1177/2045894019898368. eCollection 2020 Jan-Mar. Pulm Circ. 2020. PMID: 32292583 Free PMC article.
-
Improved long-term outcomes with catheter-directed therapies over medical management in patients with submassive pulmonary embolism-a retrospective matched cohort study.J Vasc Surg Venous Lymphat Disord. 2023 Jan;11(1):70-81. doi: 10.1016/j.jvsv.2022.09.007. Epub 2022 Oct 6. J Vasc Surg Venous Lymphat Disord. 2023. PMID: 36210021 Free PMC article.
-
American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism.Blood Adv. 2020 Oct 13;4(19):4693-4738. doi: 10.1182/bloodadvances.2020001830. Blood Adv. 2020. PMID: 33007077 Free PMC article.
References
-
- Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788–830. - PubMed
-
- Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S–94S. - PMC - PubMed
-
- Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033–69. 3069a–3069k. - PubMed
-
- Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402–11. - PubMed
-
- Healthcare Cost and Utilization Project (HCUP) Rockville M: HCUP National Inpatient Sample (NIS); 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
