

Evaluation of Timing and Route of Epinephrine in a Neonatal Model of Asphyxial Arrest
- PMID: 28214793
- PMCID: PMC5523751
- DOI: 10.1161/JAHA.116.004402
Evaluation of Timing and Route of Epinephrine in a Neonatal Model of Asphyxial Arrest
Abstract
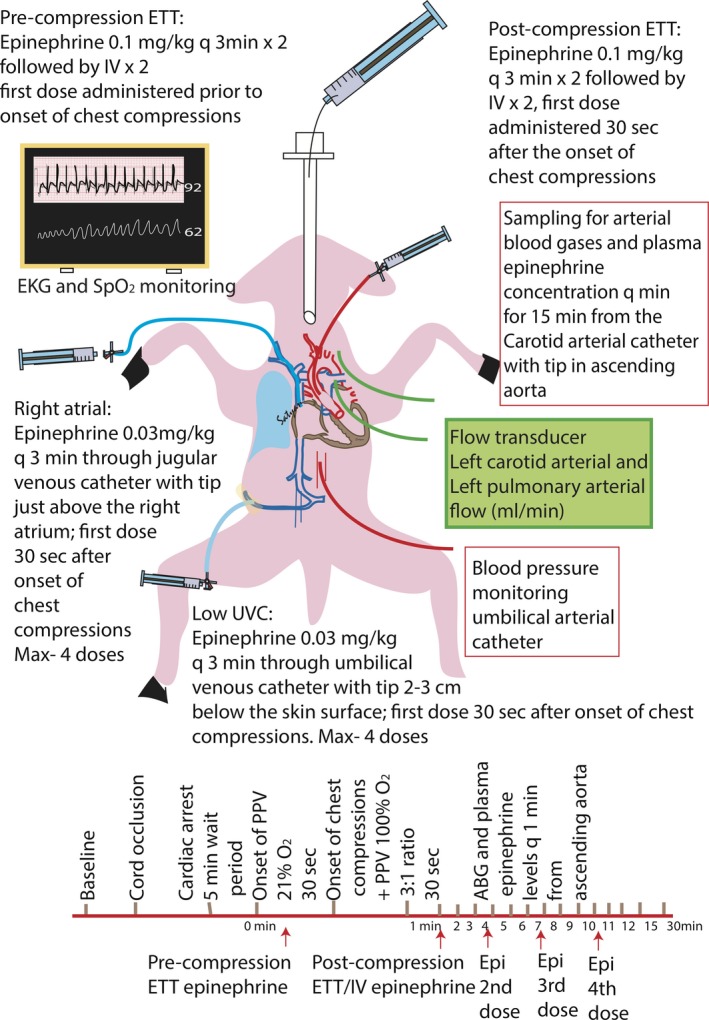
Background: Epinephrine administered by low umbilical venous catheter (UVC) or endotracheal tube (ETT) is indicated in neonates who fail to respond to positive pressure ventilation and chest compressions at birth. Pharmacokinetics of ETT epinephrine via fluid-filled lungs or UVC epinephrine in the presence of fetal shunts is unknown. We hypothesized that epinephrine administered by ETT or low UVC results in plasma epinephrine concentrations and rates of return of spontaneous circulation (ROSC) similar to right atrial (RA) epinephrine.
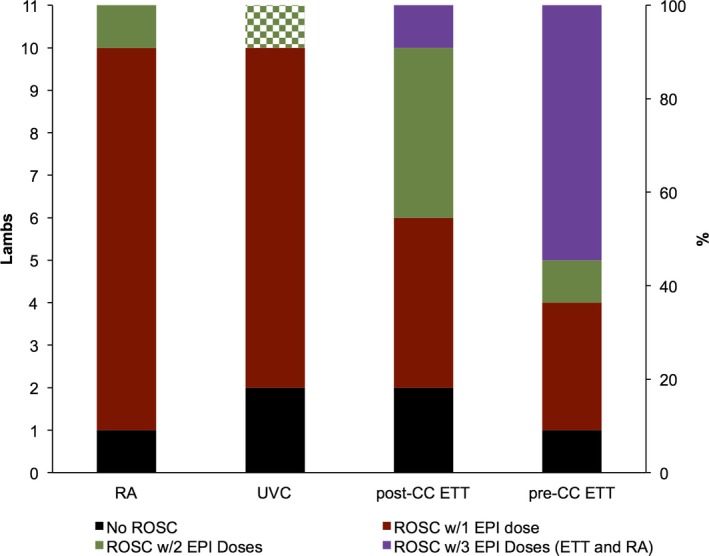
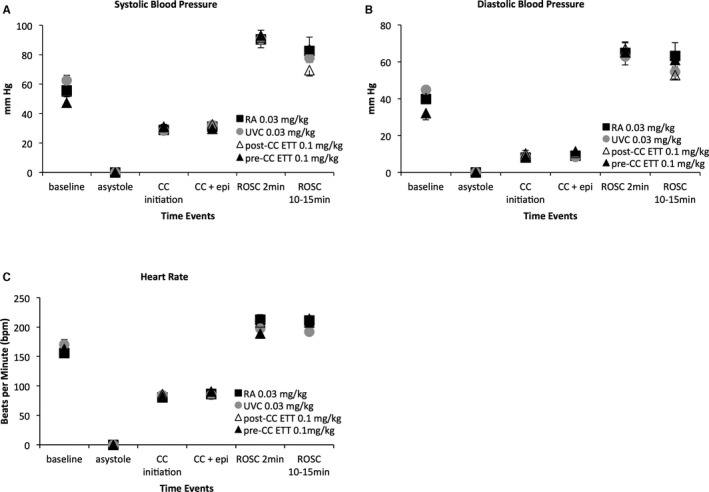
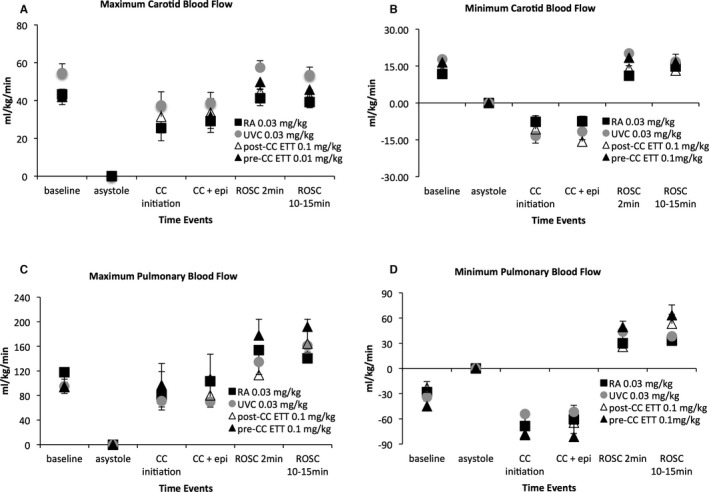
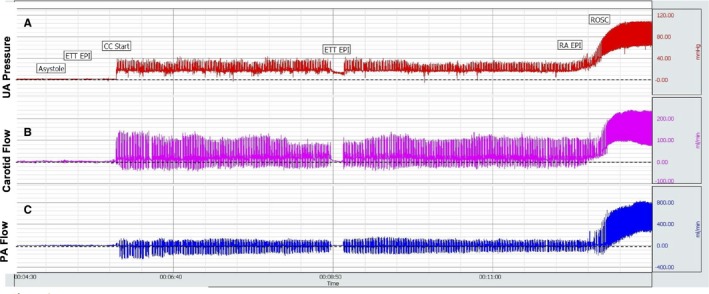
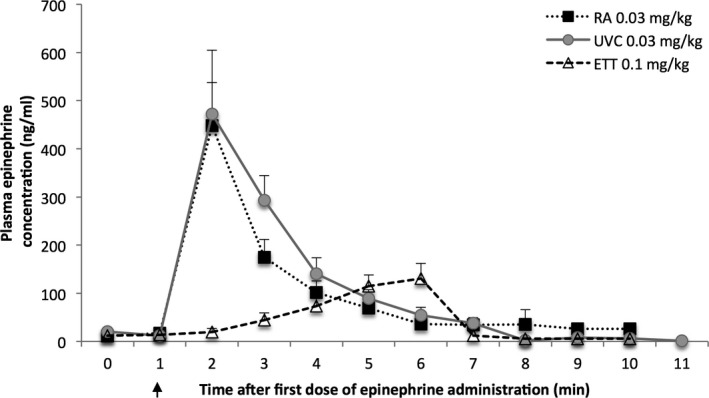
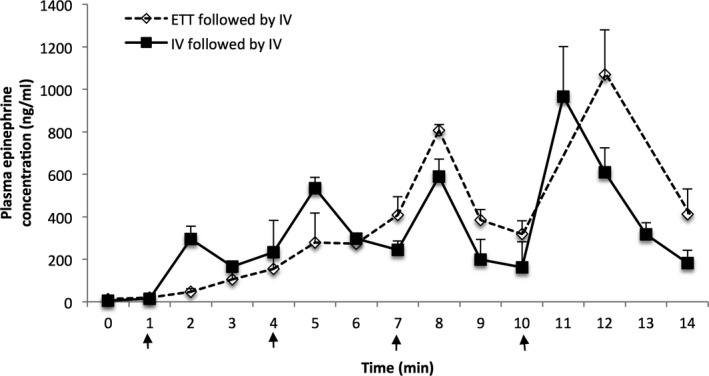
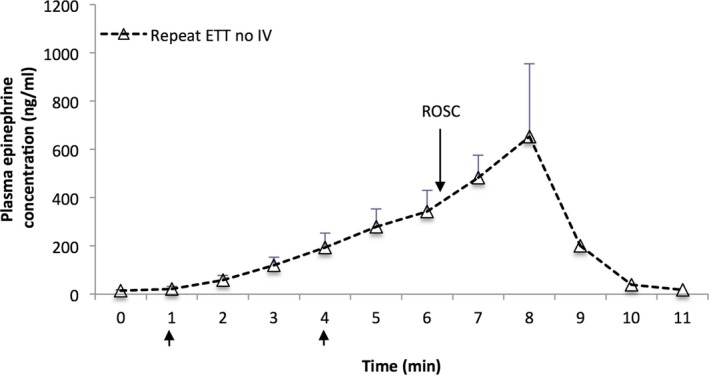
Methods and results: Forty-four lambs were randomized into the following groups: RA epinephrine (0.03 mg/kg), low UVC epinephrine (0.03 mg/kg), postcompression ETT epinephrine (0.1 mg/kg), and precompression ETT epinephrine (0.1 mg/kg). Asystole was induced by umbilical cord occlusion. Resuscitation was initiated following 5 minutes of asystole. Thirty-eight of 44 lambs achieved ROSC (10/11, 9/11, and 12/22 in the RA, UVC, and ETT groups, respectively; subsequent RA epinephrine resulted in a total ROSC of 19/22 in the ETT groups). Median time (interquartile range) to achieve ROSC was significantly longer in the ETT group (including those that received RA epinephrine) compared to the intravenous group (4.5 [2.9-7.4] versus 2 [1.9-3] minutes; P=0.02). RA and low UVC epinephrine administration achieved comparable peak plasma epinephrine concentrations (470±250 versus 450±190 ng/mL) by 1 minute compared to ETT values of 130±60 ng/mL at 5 minutes; P=0.03. Following ROSC with ETT epinephrine alone, there was a delayed peak epinephrine concentration (652±240 ng/mL).
Conclusions: The absorption of ETT epinephrine is low and delayed at birth. RA and low UVC epinephrine rapidly achieve high plasma concentrations resulting in ROSC.
Keywords: cardiac arrest; cardiac arrhythmia; epinephrine; neonate; pharmacokinetics; resuscitation.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, Jha P, Campbell H, Walker CF, Cibulskis R, Eisele T, Liu L, Mathers C; Child Health Epidemiology Reference Group of WHO and UNICEF . Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375:1969–1987. - PubMed
-
- Barber CA, Wyckoff MH. Use and efficacy of endotracheal versus intravenous epinephrine during neonatal cardiopulmonary resuscitation in the delivery room. Pediatrics. 2006;118:1028–1034. - PubMed
-
- Kapadia VS, Wyckoff MH. Drugs during delivery room resuscitation—what, when and why? Semin Fetal Neonatal Med. 2013;18:357–361. - PubMed
-
- Harrington DJ, Redman CW, Moulden M, Greenwood CE. The long‐term outcome in surviving infants with Apgar zero at 10 minutes: a systematic review of the literature and hospital‐based cohort. Am J Obstet Gynecol. 2007;196:463.e1‐5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
