

Forced Aerobic Exercise Preceding Task Practice Improves Motor Recovery Poststroke
- PMID: 28218596
- PMCID: PMC5317391
- DOI: 10.5014/ajot.2017.020297
Forced Aerobic Exercise Preceding Task Practice Improves Motor Recovery Poststroke
Abstract
Objective: To understand how two types of aerobic exercise affect upper-extremity motor recovery post-stroke. Our aims were to (1) evaluate the feasibility of having people who had a stroke complete an aerobic exercise intervention and (2) determine whether forced or voluntary exercise differentially facilitates upper-extremity recovery when paired with task practice.
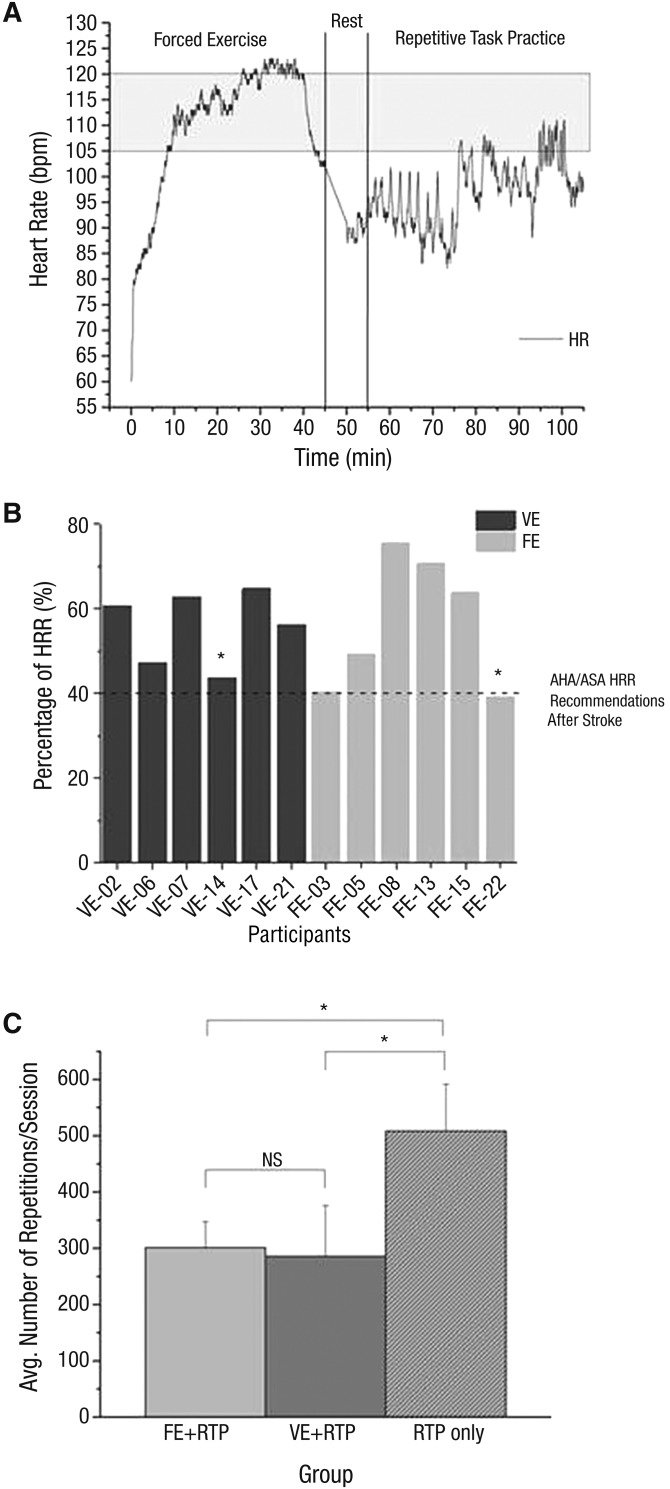
Method: Seventeen participants with chronic stroke completed twenty-four 90-min sessions over 8 wk. Aerobic exercise was immediately followed by task practice. Participants were randomized to forced or voluntary aerobic exercise groups or to task practice only.
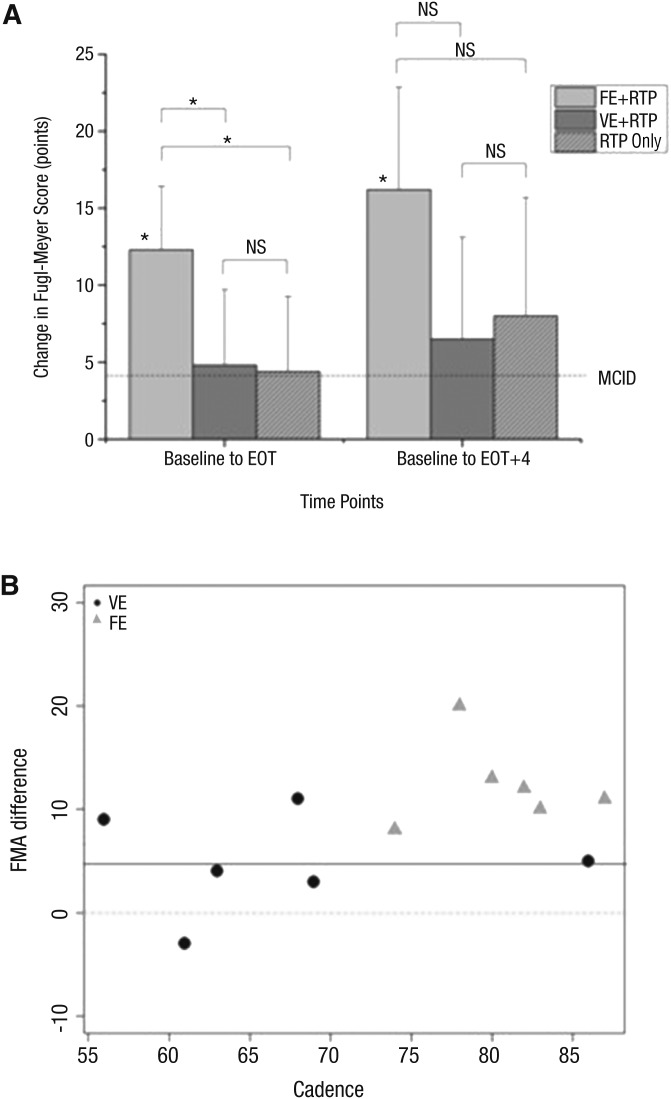
Results: Improvement on the Fugl-Meyer Assessment exceeded the minimal clinically important difference: 12.3, 4.8, and 4.4 for the forced exercise, voluntary exercise, and repetitive task practice-only groups, respectively. Only the forced exercise group exhibited a statistically significant improvement.
Conclusion: People with chronic stroke can safely complete intensive aerobic exercise. Forced aerobic exercise may be optimal in facilitating motor recovery associated with task practice.
Copyright © 2017 by the American Occupational Therapy Association, Inc.
Figures
References
-
- Alberts J. L., Linder S. M., Penko A. L., Lowe M. J., & Phillips M. (2011). It is not about the bike, it is about the pedaling: Forced exercise and Parkinson’s disease. Exercise and Sport Sciences Reviews, 39, 177–186. https://doi.org/10.1097/JES.0b013e31822cc71a - DOI - PubMed
-
- Beall E. B., Lowe M. J., Alberts J. L., Frankemolle A. M., Thota A. K., Shah C., & Phillips M. D. (2013). The effect of forced-exercise therapy for Parkinson’s disease on motor cortex functional connectivity. Brain Connectivity, 3, 190–198. https://doi.org/10.1089/brain.2012.0104 - DOI - PMC - PubMed
-
- Billinger S. A., Arena R., Bernhardt J., Eng J. J., Franklin B. A., Johnson C. M., . . . Tang A.; American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing; Council on Lifestyle and Cardiometabolic Health, Council on Epidemiology and Prevention, and Council on Clinical Cardiology. (2014). Physical activity and exercise recommendations for stroke survivors: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke, 45, 2532–2553. https://doi.org/10.1161/STR.0000000000000022 - DOI - PubMed
-
- Billinger S. A., Coughenour E., Mackay-Lyons M. J., & Ivey F. M. (2012). Reduced cardiorespiratory fitness after stroke: Biological consequences and exercise-induced adaptations. Stroke Research and Treatment, 2012, 959120 https://doi.org/10.1155/2012/959120 - DOI - PMC - PubMed
-
- Billinger S. A., Mattlage A. E., Ashenden A. L., Lentz A. A., Harter G., & Rippee M. A. (2012). Aerobic exercise in subacute stroke improves cardiovascular health and physical performance. Journal of Neurologic Physical Therapy, 36, 159–165. https://doi.org/10.1097/NPT.0b013e318274d082 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
