

Endothelial antigen assembly leads to thrombotic complications in heparin-induced thrombocytopenia
- PMID: 28218620
- PMCID: PMC5330743
- DOI: 10.1172/JCI90958
Endothelial antigen assembly leads to thrombotic complications in heparin-induced thrombocytopenia
Abstract
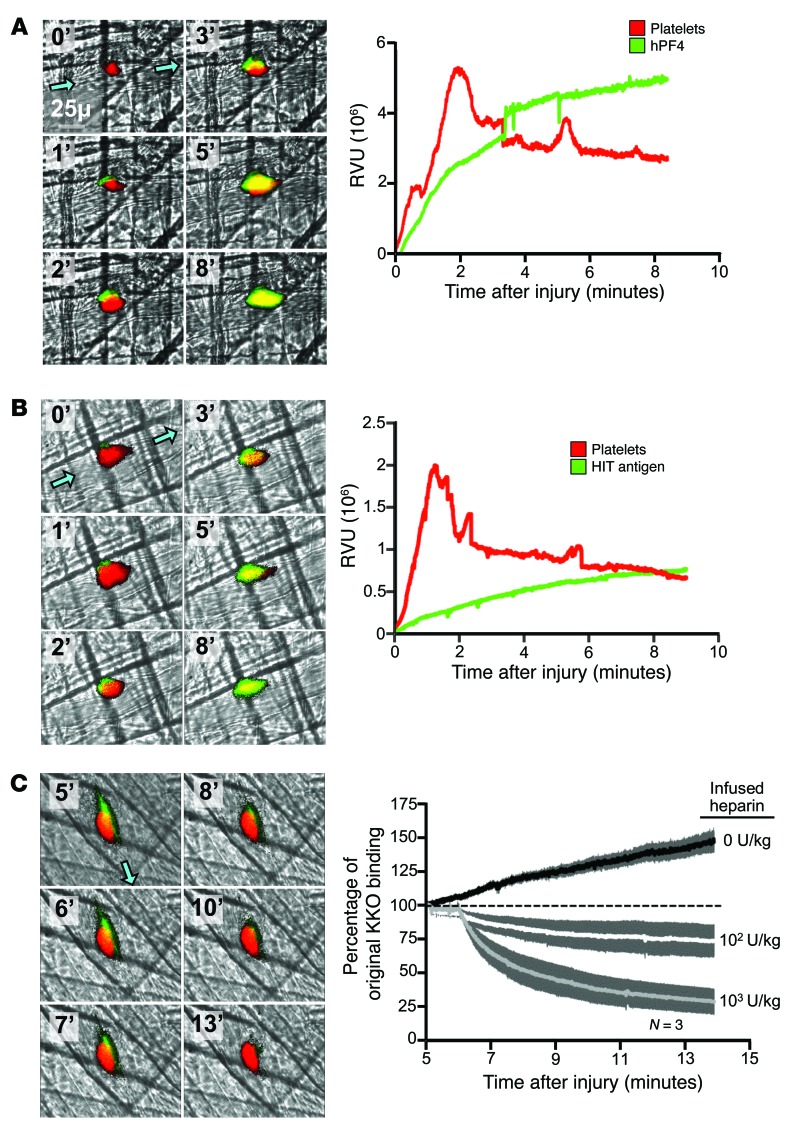
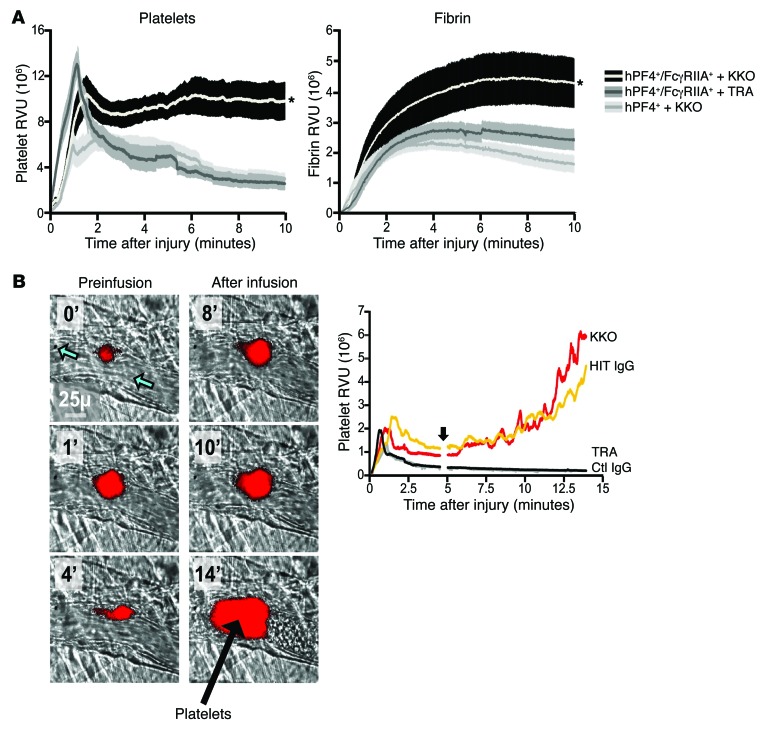
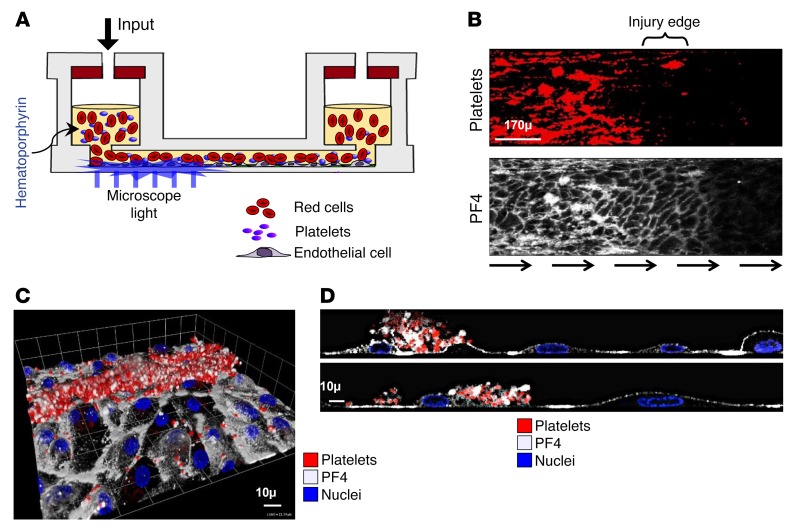
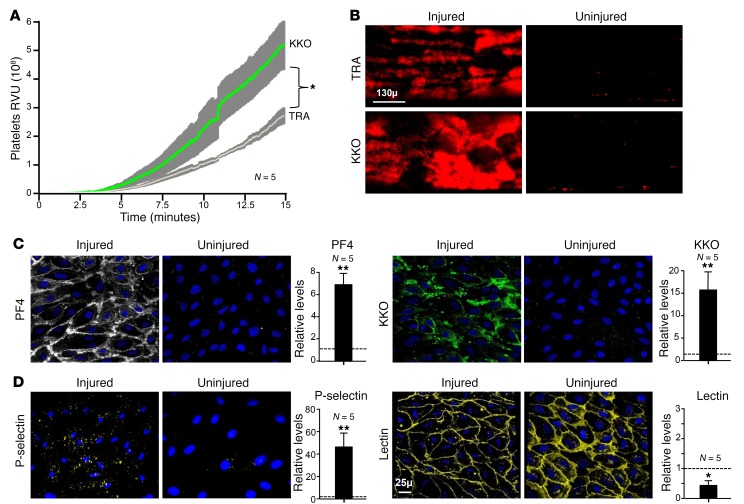
Heparin-induced thrombocytopenia (HIT) is a prothrombotic disorder initiated by antibodies against complexes between human platelet factor 4 (hPF4) and heparin. A better understanding of the events that initiate the prothrombotic state may improve approaches to antithrombotic management. Here, we visualized thrombus formation in an in vivo murine model and an endothelialized microfluidic system that simulate the pathogenesis of HIT. hPF4 released from platelets predominantly bound to peri-injury endothelium and formed HIT antigenic complexes that were dissociated by heparin. In mice expressing both hPF4+ and human platelet IgG Fc receptor IIA (FcγRIIA), infusion of the HIT-like monoclonal antibody KKO increased fibrin and platelet deposition at sites of injury, followed immediately by antigen formation on proximate endothelial cells. After a few minutes, HIT antigen was detected within the thrombus itself at the interface between the platelet core and the surrounding shell. We observed similar results in the humanized, endothelialized microfluidic system. hPF4 and KKO selectively bound to photochemically injured endothelium at sites where surface glycocalyx was reduced. These studies support the concept that the perithrombus endothelium is the predominant site of HIT antigen assembly. This suggests that disrupting antigen formation along the endothelium or protecting the endothelium may provide a therapeutic opportunity to prevent thrombotic complications of HIT, while sparing systemic hemostatic pathways.
Conflict of interest statement
Figures

References
-
- Amiral J, et al. Platelet factor 4 complexed to heparin is the target for antibodies generated in heparin-induced thrombocytopenia. Thromb Haemost. 1992;68(1):95–96. - PubMed
-
- Greinacher A, Farner B, Kroll H, Kohlmann T, Warkentin TE, Eichler P. Clinical features of heparin-induced thrombocytopenia including risk factors for thrombosis. A retrospective analysis of 408 patients. Thromb Haemost. 2005;94(1):132–135. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
