

Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria
- PMID: 28219327
- PMCID: PMC5319106
- DOI: 10.1186/s12882-017-0487-8
Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria
Abstract
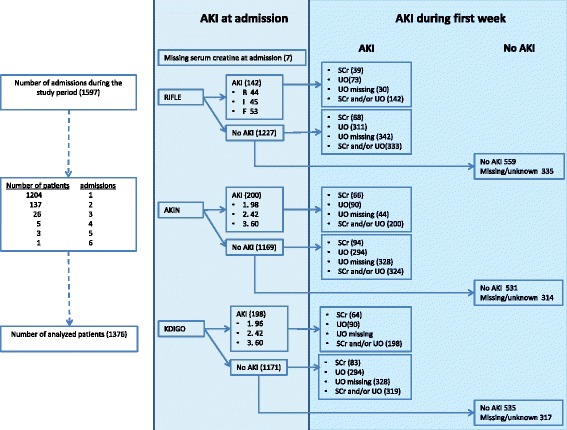
Background: Acute kidney injury (AKI) is a serious complication of critical illness with both attributed morbidity and mortality at short-term and long-term. The incidence of AKI reported in critically ill patients varies substantially with the population evaluated and the definitions used. We aimed to assess which of the AKI definitions (RIFLE, AKIN or KDIGO) with or without urine output criteria recognizes AKI most frequently and quickest. Additionally, we conducted a review on the comparison of incidence proportions of varying AKI definitions in populations of critically ill patients.
Methods: We included all patients with index admissions to our intensive care unit (ICU) from January 1st, 2014 until June 11th, 2014 to determine the incidence and onset of AKI by RIFLE, AKIN and KDIGO during the first 7 days of ICU admission. We conducted a sensitive search using PubMed evaluating the comparison of RIFLE, AKIN and KDIGO in critically ill patients RESULTS: AKI incidence proportions were 15, 21 and 20% respectively using serum creatinine criteria of RIFLE, AKIN and KDIGO. Adding urine output criteria increased AKI incidence proportions to 35, 38 and 38% using RIFLE, AKIN and KDIGO definitions. Urine output criteria detected AKI in patients without AKI at ICU admission in a median of 13 h (IQR 7-22 h; using RIFLE definition) after admission compared to a median of 24 h using serum creatinine criteria (IQR24-48 h). In the literature a large heterogeneity exists in patients included, AKI definition used, reference or baseline serum creatinine used, and whether urine output in the staging of AKI is used.
Conclusion: AKIN and KDIGO criteria detect more patients with AKI compared to RIFLE criteria. Addition of urine output criteria detect patients with AKI 11 h earlier than serum creatinine criteria and may double AKI incidences in critically ill patients. This could explain the large heterogeneity observed in literature.
Keywords: Acute kidney injury; Definitions; Incidence; Intensive Care; Timing.
Figures

References
-
- Gammelager H, Christiansen CF, Johansen MB, Tonnesen E, Jespersen B, Sorensen HT. Five-year risk of end-stage renal disease among intensive care patients surviving dialysis-requiring acute kidney injury: a nationwide cohort study. Crit Care. 2013;17(4):R145. doi: 10.1186/cc12824. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
