

Molecular and genetic alterations associated with therapy resistance and relapse of acute myeloid leukemia
- PMID: 28219393
- PMCID: PMC5322789
- DOI: 10.1186/s13045-017-0416-0
Molecular and genetic alterations associated with therapy resistance and relapse of acute myeloid leukemia
Abstract
Background: The majority of individuals with acute myeloid leukemia (AML) respond to initial chemotherapy and achieve a complete remission, yet only a minority experience long-term survival because a large proportion of patients eventually relapse with therapy-resistant disease. Relapse therefore represents a central problem in the treatment of AML. Despite this, and in contrast to the extensive knowledge about the molecular events underlying the process of leukemogenesis, information about the mechanisms leading to therapy resistance and relapse is still limited.
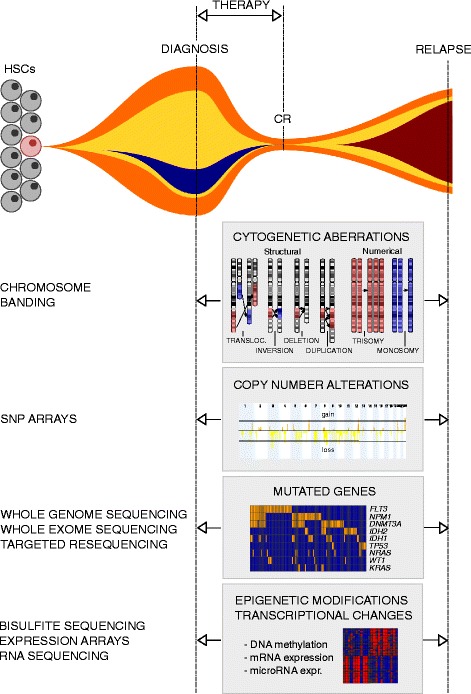
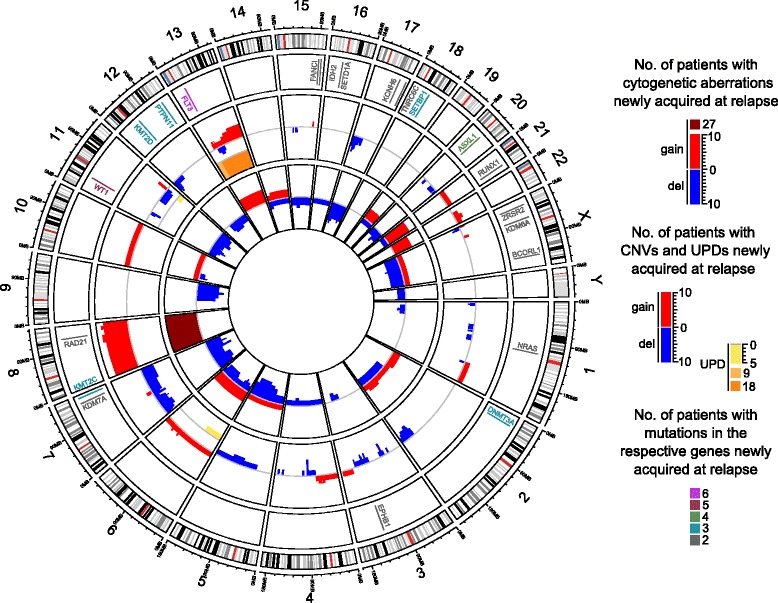
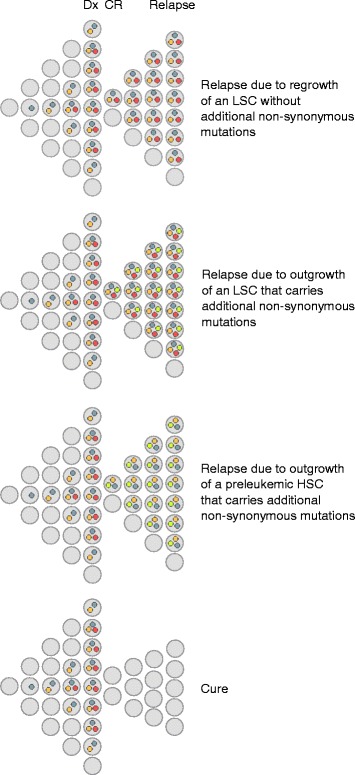
Purpose and content of review: Recently, a number of studies have aimed to fill this gap and provided valuable information about the clonal composition and evolution of leukemic cell populations during the course of disease, and about genetic, epigenetic, and gene expression changes associated with relapse. In this review, these studies are summarized and discussed, and the data reported in them are compiled in order to provide a resource for the identification of molecular aberrations recurrently acquired at, and thus potentially contributing to, disease recurrence and the associated therapy resistance. This survey indeed uncovered genetic aberrations with known associations with therapy resistance that were newly gained at relapse in a subset of patients. Furthermore, the expression of a number of protein coding and microRNA genes was reported to change between diagnosis and relapse in a statistically significant manner.
Conclusions: Together, these findings foster the expectation that future studies on larger and more homogeneous patient cohorts will uncover pathways that are robustly associated with relapse, thus representing potential targets for rationally designed therapies that may improve the treatment of patients with relapsed AML, or even facilitate the prevention of relapse in the first place.
Keywords: Acute myeloid leukemia; Clonal evolution; Copy number variation; Cytogenetics; DNA methylation; Gene expression profiling; Relapse; Single nucleotide variants; Therapy resistance.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
