

Putting 3D modelling and 3D printing into practice: virtual surgery and preoperative planning to reconstruct complex post-traumatic skeletal deformities and defects
- PMID: 28220752
- PMCID: PMC5319375
- DOI: 10.1051/sicotj/2016043
Putting 3D modelling and 3D printing into practice: virtual surgery and preoperative planning to reconstruct complex post-traumatic skeletal deformities and defects
Abstract
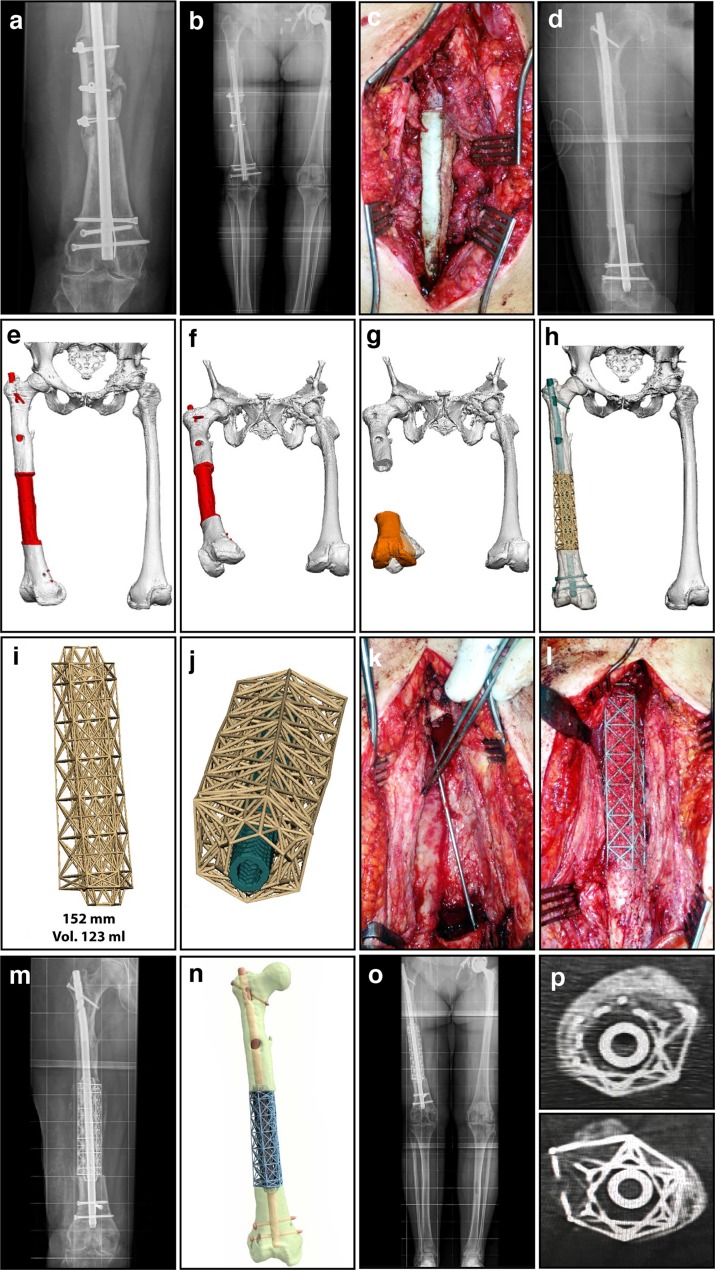
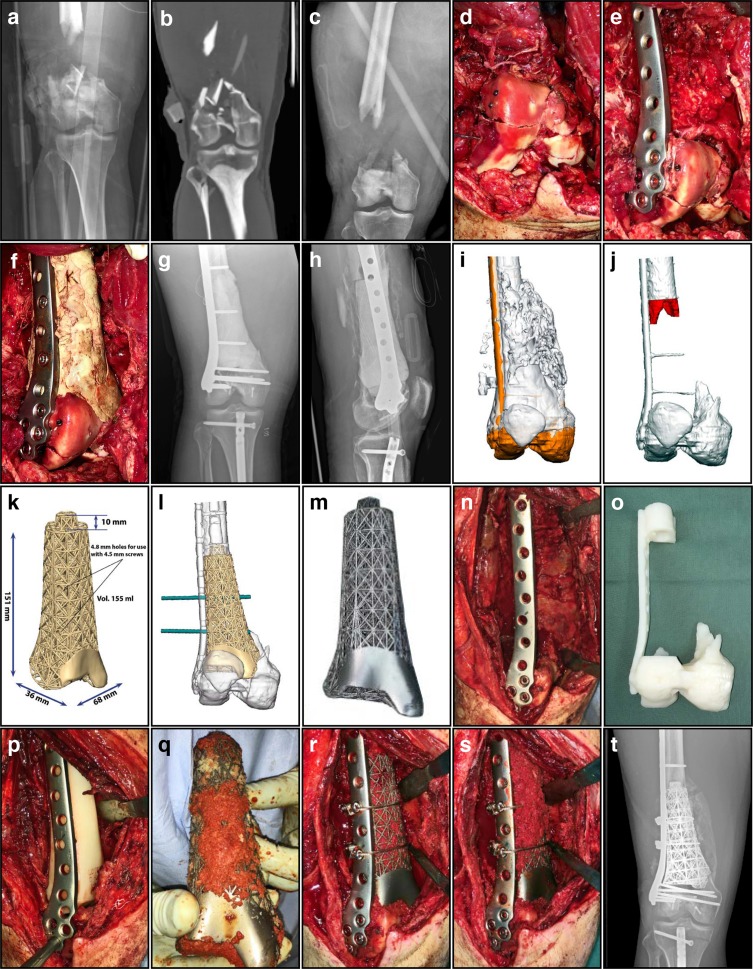
3D printing technology has revolutionized and gradually transformed manufacturing across a broad spectrum of industries, including healthcare. Nowhere is this more apparent than in orthopaedics with many surgeons already incorporating aspects of 3D modelling and virtual procedures into their routine clinical practice. As a more extreme application, patient-specific 3D printed titanium truss cages represent a novel approach for managing the challenge of segmental bone defects. This review illustrates the potential indications of this innovative technique using 3D printed titanium truss cages in conjunction with the Masquelet technique. These implants are custom designed during a virtual surgical planning session with the combined input of an orthopaedic surgeon, an orthopaedic engineering professional and a biomedical design engineer. The ability to 3D model an identical replica of the original intact bone in a virtual procedure is of vital importance when attempting to precisely reconstruct normal anatomy during the actual procedure. Additionally, other important factors must be considered during the planning procedure, such as the three-dimensional configuration of the implant. Meticulous design is necessary to allow for successful implantation through the planned surgical exposure, while being aware of the constraints imposed by local anatomy and prior implants. This review will attempt to synthesize the current state of the art as well as discuss our personal experience using this promising technique. It will address implant design considerations including the mechanical, anatomical and functional aspects unique to each case.
© The Authors, published by EDP Sciences, 2017.
Figures
References
-
- Grant CA, Izatt MT, Labrom RD, Askin GN, Glatt V (2016) Use of 3D printing in complex spinal surgery: historical perspectives, current usage, and future directions. Tech Orthop 31(3), 172–180.
-
- Green N, Glatt V, Tetsworth K, Wilson LJ, Grant CA (2016) A practical guide to image processing in the creation of 3d models for orthopedics. Tech Orthop 31(3), 153–163.
-
- Kalamaras M, McEniery P, Thorn K, Bindra R (2016) Rapid prototyping and 3D modeling of osteotomy jigs and drill guides in hand and wrist surgery. Tech Orthop 31(3), 164–171.
-
- Tetsworth K (2016) Three-dimensional modeling, rapid prototypes, and additive manufacturing: the diffusion of innovation and the adoption of technology in orthopedic surgery. Tech Orthop 31(3), 141–142.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials