

Pulmonary outcomes following specialized respiratory management for acute cervical spinal cord injury: a retrospective analysis
- PMID: 28220822
- PMCID: PMC5457341
- DOI: 10.1038/sc.2017.10
Pulmonary outcomes following specialized respiratory management for acute cervical spinal cord injury: a retrospective analysis
Abstract
Study design: Retrospective analysis.
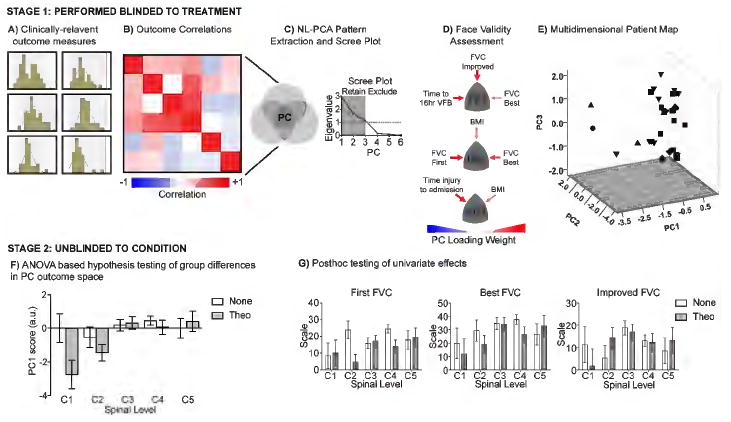
Objectives: To identify multivariate interactions of respiratory function that are sensitive to spinal cord injury level and pharmacological treatment to promote strategies that increase successful liberation from mechanical ventilation.
Setting: United States regional spinal cord injury (SCI) treatment center.
Methods: Retrospective chart review of patients consecutively admitted to Santa Clara Valley Medical Center between May 2013 and December 2014 for ventilator weaning with C1-C5 American Spinal Injury Association Impairment Scale (AIS) A or B SCI, <3 months from injury and who had a tracheostomy in place. A nonlinear, categorical principal component analysis (NL-PCA) was performed to test the multivariate interaction of respiratory outcomes from patients (N=36) being weaned off ventilator support after acute SCI with (N=15) or without (N=21) theophylline treatment.
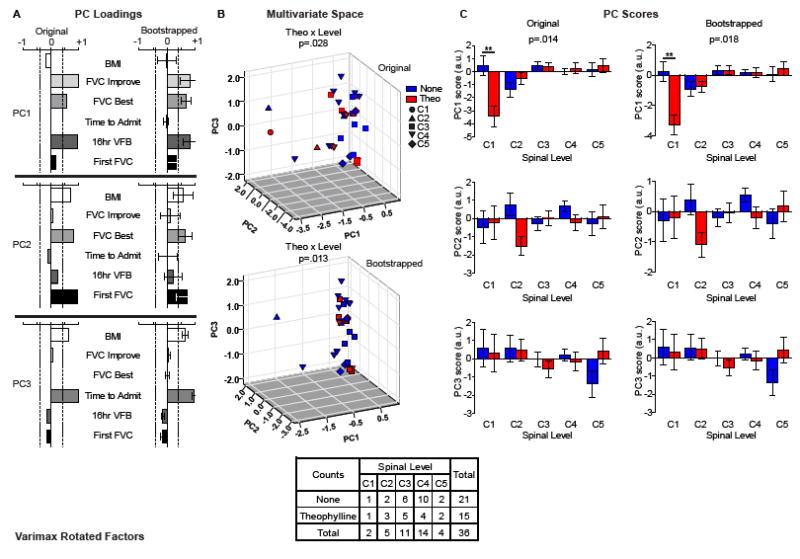
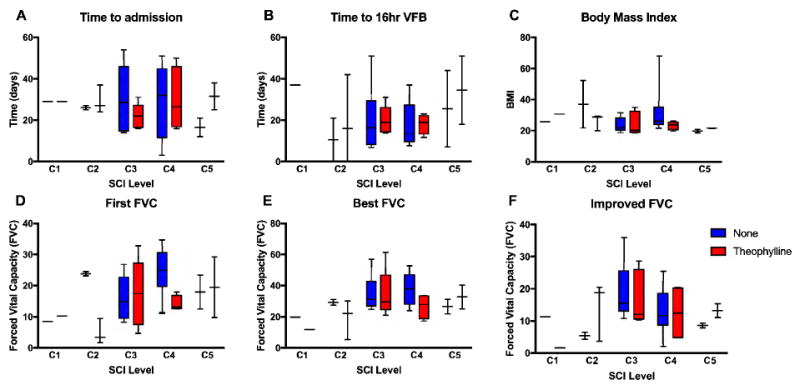
Results: In total, 36 patients met inclusion criteria (2 C1, 5 C2, 11 C3, 14 C4 and 4 C5). The NL-PCA returned three independent components that accounted for 95% of the variance in the data set. Multivariate general linear models hypothesis tests revealed a significant syndromic interaction between theophylline treatment and SCI level (Wilks' Lambda, P=0.028, F (12,64)=2.116, η2=0.256, 1-β=0.838), with post hoc testing demonstrating a significant interaction on PC1, explained by a positive correlation between improved forced vital capacity and time it took to reach 16 h of ventilator-free breathing. Thirty-three patients (92%) achieved 16 h of ventilator-free breathing (VFB) and 30 patients (83%) achieved 24 h of VFB.
Conclusions: We suspect that some portion of the high success rate of ventilator weaning may be attributable to theophylline use in higher cervical SCI, in addition to our aggressive regimen of high volume ventilation, medication optimization and pulmonary toilet (positive pressure treatments and mechanical insufflation-exsufflation).
Conflict of interest statement
The authors declare no conflict of interests.
Figures
References
-
- National Spinal Cord Injury Statistical Center. Facts and Figures at a Glance. 2015 [Internet] Available from: https://http://www.nscisc.uab.edu/PublicDocuments/fact_figures_docs/Fact....
-
- Posluszny JA, Onders R, Kerwin AJ, Weinstein MS, Stein DM, Knight J, et al. Multicenter review of diaphragm pacing in spinal cord injury: successful not only in weaning from ventilators but also in bridging to independent respiration. J Trauma Acute Care Surg. 2014;76(2):303–9. discussion 9-10. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
