

Clinical Investigation of the Posterior scleral contraction to Treat Macular Traction Maculopathy in Highly Myopic Eyes
- PMID: 28220890
- PMCID: PMC5318876
- DOI: 10.1038/srep43256
Clinical Investigation of the Posterior scleral contraction to Treat Macular Traction Maculopathy in Highly Myopic Eyes
Abstract
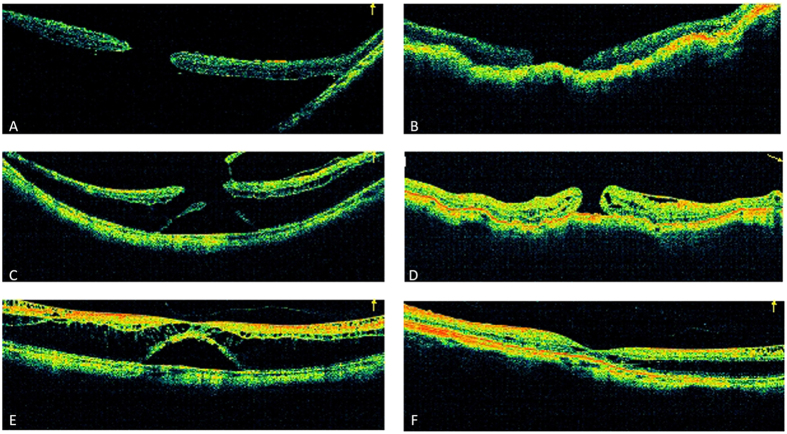
Myopic traction maculopathy (MTM) can cause vision disabilities in highly myopic eyes. This retrospective case series investigated the clinical outcomes of posterior scleral contraction (PSC) using genipin-cross-linked sclera as the material to treat MTM in highly myopic eyes. In total, 32 eyes from 29 highly myopic patients who underwent PSC for MTM were recruited. The changes in best-corrected visual acuity (BCVA) and axial length were evaluated, macular reattachment and macular hole (MH) closure was assessed by optical coherence tomography, and complications were evaluated. At the final follow-up, the retina was completely reattached in 25 eyes (78.1%), essentially reattached in 4 eyes (12.5%), and partially reattached in 3 eyes (9.4%). The logMAR BCVA improved significantly from 1.18 ± 0.45 preoperatively to 0.87 ± 0.45 postoperatively (P < 0.001). The 32 eyes were further divided into the MH group (16 eyes) and the non-MH group (16 eyes) for comparison. The MH was closed in 9 eyes (56.3%). The retinal reattachment rate was 75.0% in the MH group and 81.25% in the non-MH group, and the logMAR BCVA improved significantly in both groups. The PSC using genipin-cross-linked sclera as the material can effectively treat MTM in highly myopic eyes, and significant visual improvement can be achieved with minimal complications.
Conflict of interest statement
The authors declare no competing financial interests.
Figures

References
-
- Buch H., Vinding T. & Nielsen N. V. Prevalence and causes of visual impairment according to World Health Organization and United States criteria in an aged, urban Scandinavian population: the Copenhagen City Eye Study. Ophthalmology 108, 2347–2357 (2001). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
