

Light and energy based therapeutics for genitourinary syndrome of menopause: Consensus and controversies
- PMID: 28220946
- PMCID: PMC5819602
- DOI: 10.1002/lsm.22637
Light and energy based therapeutics for genitourinary syndrome of menopause: Consensus and controversies
Abstract
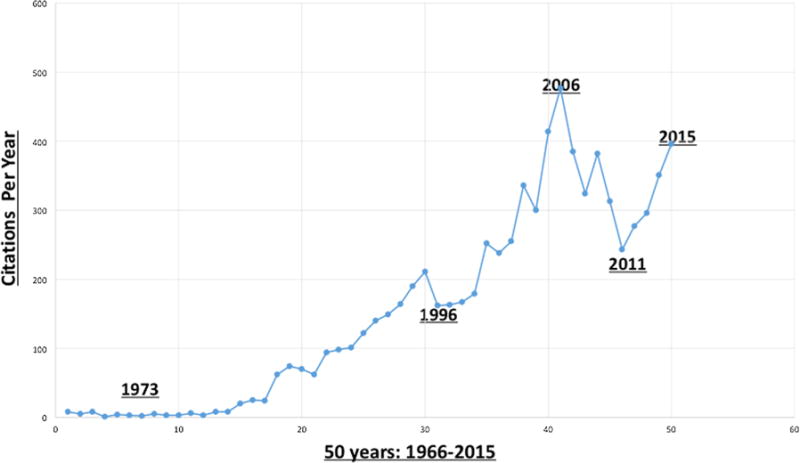
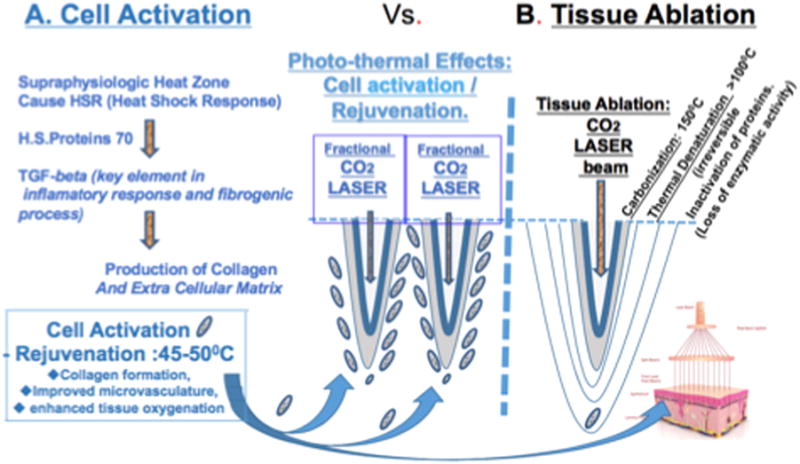
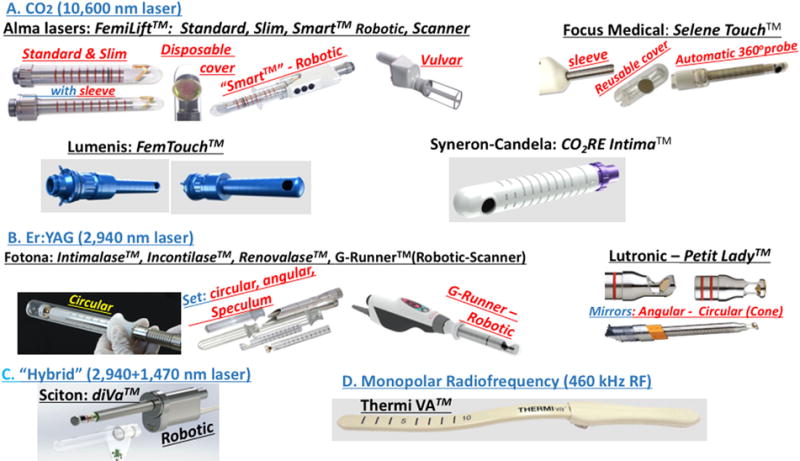
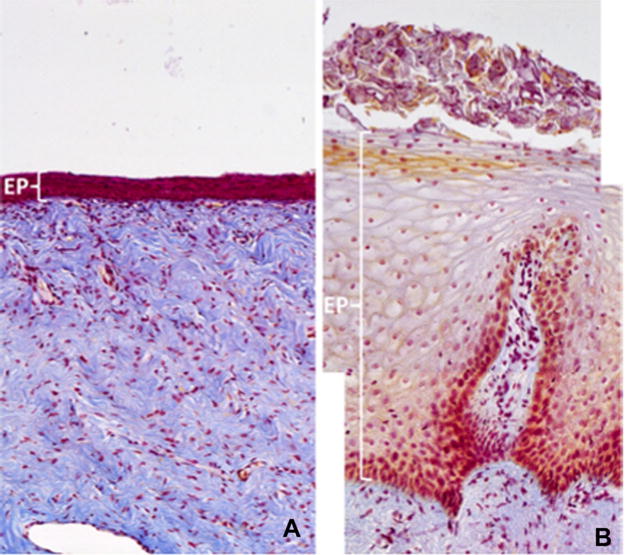
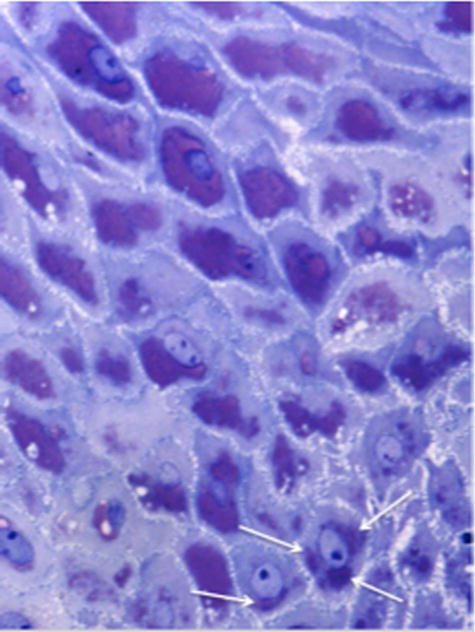
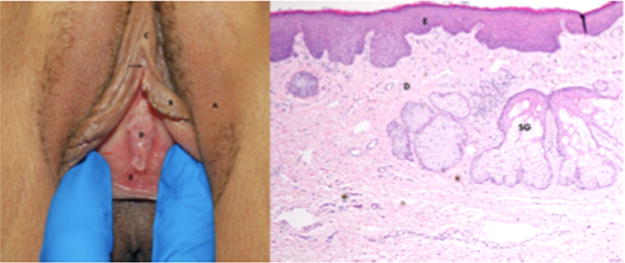
Gynecologist and plastic surgeons pioneered the application of lasers in medicine and surgery almost 5 decades ago, initially used to treat cervical and vaginal pathologies. Ever since, energy-based devices have been deployed to treat pelvic pathologies and improve fertility. Recent technological developments triggered an unprecedented wave of publications, assessing the efficacy of fractional laser, and radiofrequency on the vaginal wall in reversing natural aging processes. Studies have shown that a certain degree of thermal energy deposited on the vaginal wall stimulates proliferation of the glycogen-enriched epithelium, neovascularization, and collagen formation in the lamina propria, and improves natural lubrication and control of urination. This review aimed to review such data and to guide future research. A unique assembly of experts from around the globe, compiled and edited this manuscript based on a thorough literature review and personal experience. Lasers Surg. Med. 49:137-159, 2017. © 2017 Wiley Periodicals, Inc.
Keywords: energy based device; genitourinary syndrome of menopause (GSM); laser; lichen sclerosus; vulvodynia; radiofrequency; rejuvenation; stress urinary incontinence (SUI); vagina; vulva.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
Conflict of Interest Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and have disclosed the following: Yona Tadir is a scientific consultant for Alma Lasers. Red Alinsod is a consultant for Thermi, receive royalty for ThermiVa, Cooper Surgical, Lone Star Retractor, and Coloplast. Consultant, Caldera Medical: Stock owner, Monarch Medical Products: Consultant, Royalty for Alinsod Surgical Equipment. Selih-Martinec K. is an invited speaker by Alma Lasers. Alberto Calligaro, Stefano Salvatore, and Nicola Zerbinati are scientific consultants for DEKA laser. All other co-authors: nothing to disclose. No commercial source supported the collaboration and preparation of this manuscript.
Figures





References
-
- Kaplan I, Goldman J, Ger R. The treatment of erosions of the uterine cervix by means of the CO2 laser. Obstet Gynecol. 1973;41(5):795–796. - PubMed
-
- Bellina JH, Polanyi TG. Management of vaginal adenosis and related cervico-vaginal disorders in DES-exposed pregnancy by means of carbon dioxide laser surgery. J Reprod Med. 1976;16:295–296. - PubMed
-
- Bruhat M, Mage G, Mahnes M. Use of the CO2 laser in laparoscopy. Proceedings of the 3rd international society for laser surgery. Ed. Kaplan I. 1979;24:235–238.
-
- Tadir Y, Kaplan I, Zukerman Z, Ovadia J. Laparoscopic CO2 laser sterilization. In: Semm K, Mettler L, editors. Human Reproduction. Exerpta Medica, Amsterdam: Elsevier; 1981. pp. 551pp. 423–431.
-
- Nezhat FR, Nezhat CR, Silfen SL. Videolaseroscopy for oophorectomy. Am J Obstet Gynecol. 1991;165:1323–1330. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
