

Antipyretic Therapy in Critically Ill Septic Patients: A Systematic Review and Meta-Analysis
- PMID: 28221185
- PMCID: PMC5389594
- DOI: 10.1097/CCM.0000000000002285
Antipyretic Therapy in Critically Ill Septic Patients: A Systematic Review and Meta-Analysis
Abstract
Objective: This meta-analysis aimed to examine the impact of antipyretic therapy on mortality in critically ill septic adults.
Data sources: Literature searches were implemented in Ovid Medline, Embase, Scopus, Cumulative Index of Nursing and Allied Health Literature, Cochrane Central Register of Controlled Trials, NHS Economic Evaluation Database, and ClinicalTrials.gov through February 2016.
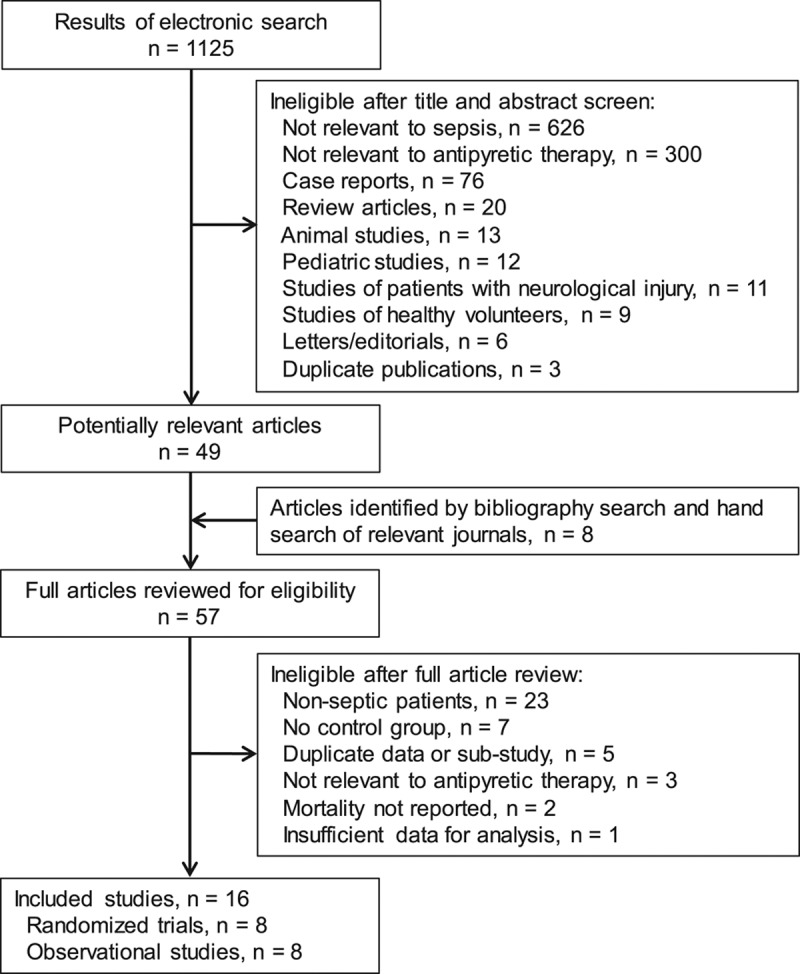
Study selection: Inclusion criteria were observational or randomized studies of septic patients, evaluation of antipyretic treatment, mortality reported, and English-language version available. Studies were excluded if they enrolled pediatric patients, patients with neurologic injury, or healthy volunteers. Criteria were applied by two independent reviewers.
Data extraction: Two reviewers independently extracted data and evaluated methodologic quality. Outcomes included mortality, frequency of shock reversal, acquisition of nosocomial infections, and changes in body temperature, heart rate, and minute ventilation. Randomized and observational studies were analyzed separately.
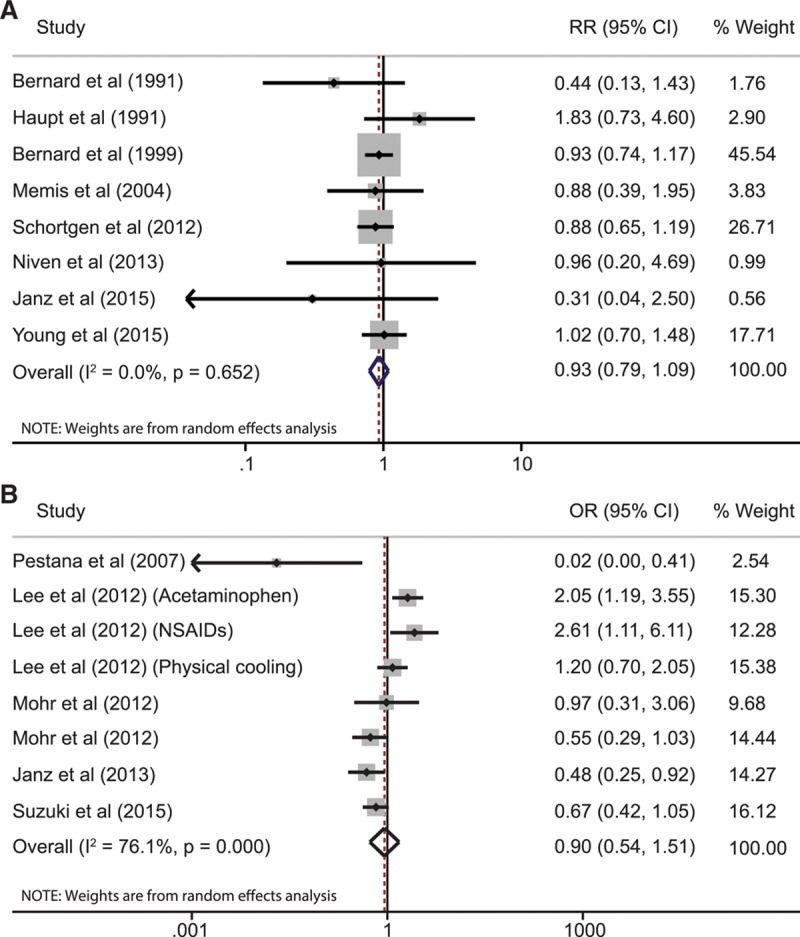
Data synthesis: Eight randomized studies (1,507 patients) and eight observational studies (17,432 patients) were analyzed. Antipyretic therapy did not reduce 28-day/hospital mortality in the randomized studies (relative risk, 0.93; 95% CI, 0.77-1.13; I = 0.0%) or observational studies (odds ratio, 0.90; 95% CI, 0.54-1.51; I = 76.1%). Shock reversal (relative risk, 1.13; 95% CI, 0.68-1.90; I = 51.6%) and acquisition of nosocomial infections (relative risk, 1.13; 95% CI, 0.61-2.09; I = 61.0%) were also unchanged. Antipyretic therapy decreased body temperature (mean difference, -0.38°C; 95% CI, -0.63 to -0.13; I = 84.0%), but not heart rate or minute ventilation.
Conclusions: Antipyretic treatment does not significantly improve 28-day/hospital mortality in adult patients with sepsis.
Figures
Comment in
-
Does Antipyresis Improve Mortality in Critically Ill Septic Patients?Ann Emerg Med. 2017 Oct;70(4):573-575. doi: 10.1016/j.annemergmed.2017.05.010. Epub 2017 Jun 27. Ann Emerg Med. 2017. PMID: 28662912 No abstract available.
References
-
- Lagu T, Rothberg MB, Shieh MS, et al. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med 2012; 40:754–761 - PubMed
-
- Young PJ, Saxena M, Beasley R, et al. Early peak temperature and mortality in critically ill patients with or without infection. Intensive Care Med 2012; 38:437–444. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
