

Cost-Effectiveness of Immune Checkpoint Inhibition in BRAF Wild-Type Advanced Melanoma
- PMID: 28221865
- PMCID: PMC5791832
- DOI: 10.1200/JCO.2016.69.6336
Cost-Effectiveness of Immune Checkpoint Inhibition in BRAF Wild-Type Advanced Melanoma
Abstract
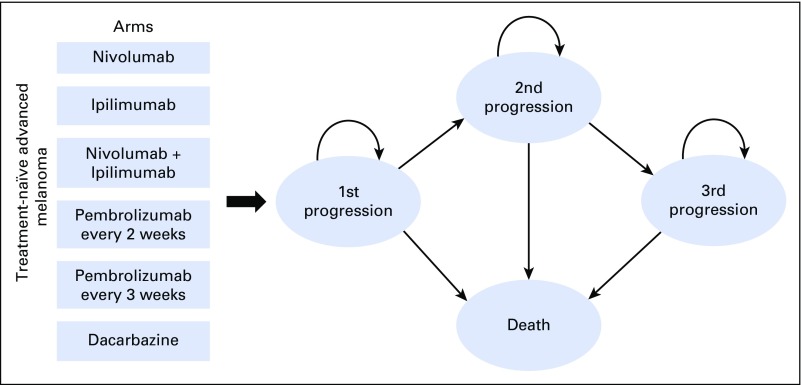
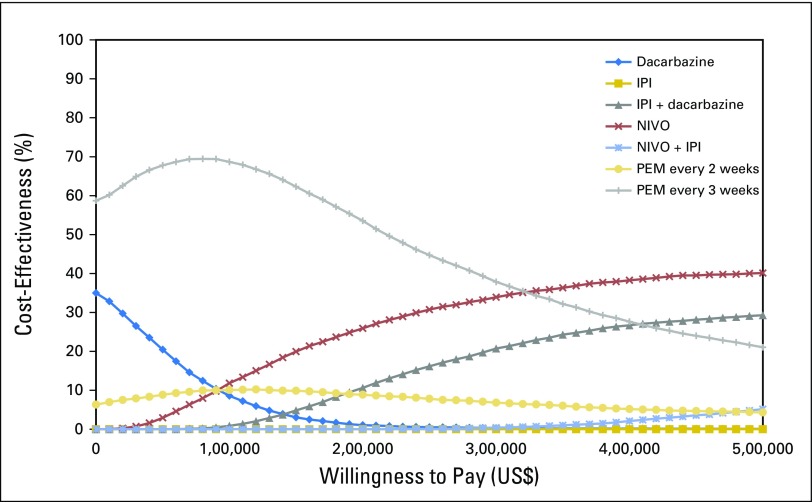
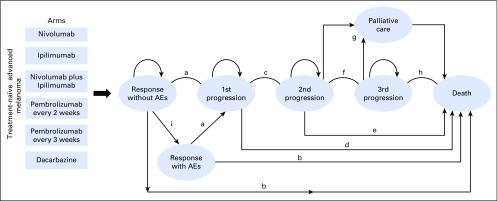
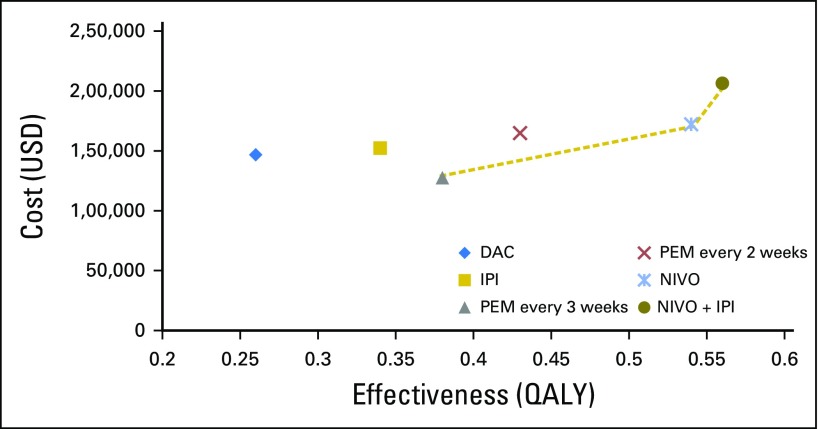
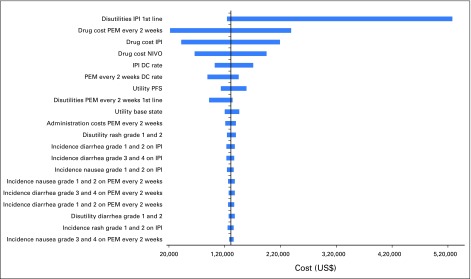
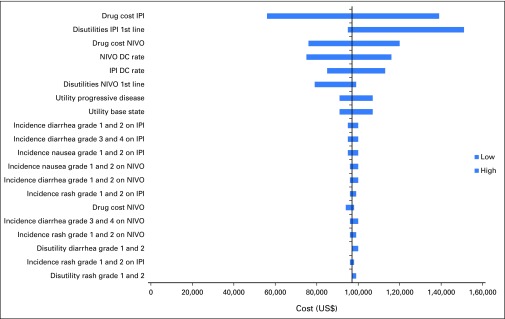
Purpose Patients who are diagnosed with stage IV metastatic melanoma have an estimated 5-year relative survival rate of only 17%. Randomized controlled trials of recent US Food and Drug Administration-approved immune checkpoint inhibitors-pembrolizumab (PEM), nivolumab (NIVO), and ipilumumab (IPI)-demonstrate improved patient outcomes, but the optimal treatment sequence in patients with BRAF wild-type metastatic melanoma remains unclear. To inform policy makers about the value of these treatments, we developed a Markov model to compare the cost-effectiveness of different strategies for sequencing novel agents for the treatment of advanced melanoma. Materials and Methods We developed Markov models by using a US-payer perspective and lifetime horizon to estimate costs (2016 US$) and quality-adjusted life years (QALYs) for treatment sequences with first-line NIVO, IPI, NIVO + IPI, PEM every 2 weeks, and PEM every 3 weeks. Health states were defined for initial treatment, first and second progression, and death. Rates for drug discontinuation, frequency of adverse events, disease progression, and death obtained from randomized phase III trials were used to determine the likelihood of transition between states. Deterministic and probabilistic sensitivity analyses were conducted to evaluate model uncertainty. Results PEM every 3 weeks followed by second-line IPI was both more effective and less costly than dacarbazine followed by IPI then NIVO, or IPI followed by NIVO. Compared with the first-line dacarbazine treatment strategy, NIVO followed by IPI produced an incremental cost effectiveness ratio of $90,871/QALY, and first-line NIVO + IPI followed by carboplatin plus paclitaxel chemotherapy produced an incremental cost effectiveness ratio of $198,867/QALY. Conclusion For patients with treatment-naive BRAF wild-type advanced melanoma, first-line PEM every 3 weeks followed by second-line IPI or first-line NIVO followed by second-line IPI are the most cost-effective, immune-based treatment strategies for metastatic melanoma.
Figures
Comment in
-
Comprehensive Reporting in Cost-Effectiveness Modeling.J Clin Oncol. 2017 Sep 10;35(26):3085-3086. doi: 10.1200/JCO.2017.73.6355. Epub 2017 Jul 17. J Clin Oncol. 2017. PMID: 28715247 No abstract available.
-
Reply to Á. Benedict et al.J Clin Oncol. 2017 Sep 10;35(26):3086-3087. doi: 10.1200/JCO.2017.74.5273. Epub 2017 Jul 17. J Clin Oncol. 2017. PMID: 28715248 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- American Cancer Society Cancer treatment & survivorship facts & figures 2016-2017. http://www.cancer.org/acs/groups/content/@research/documents/document/ac...
-
- Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975–2012. http://seer.cancer.gov/csr/1975_2010/
-
- Long GV, Menzies AM, Nagrial AM, et al. Prognostic and clinicopathologic associations of oncogenic BRAF in metastatic melanoma. J Clin Oncol. 2011;29:1239–1246. - PubMed
-
- Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–954. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
